
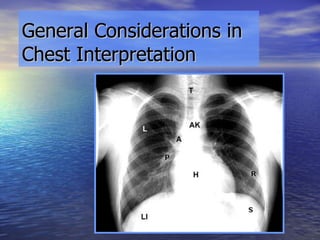

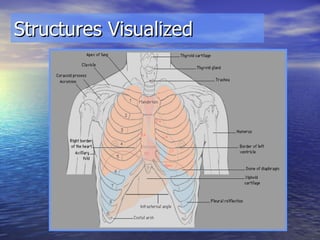
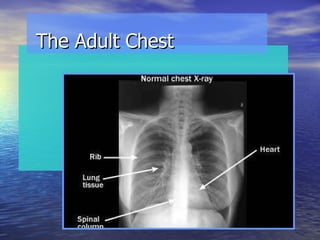
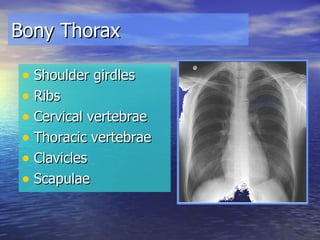
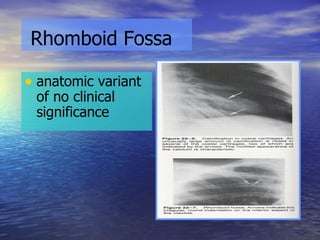
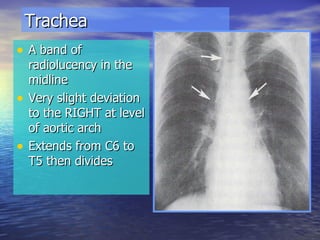


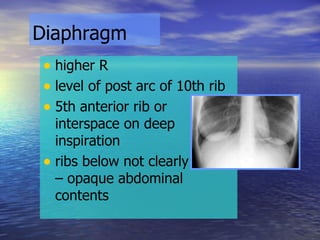
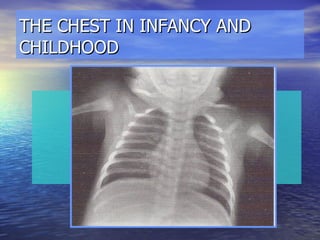


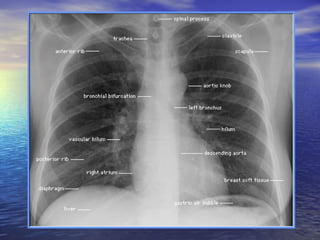


This document provides an overview of how to interpret a normal chest x-ray by describing the anatomical structures that should be visualized and what is considered normal for each structure. It discusses evaluating the bony thorax, soft tissues, mediastinum, lungs and diaphragm and how they change with age from infancy to childhood to older age. Key anatomical structures and their expected appearance on a normal chest x-ray are defined.































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











