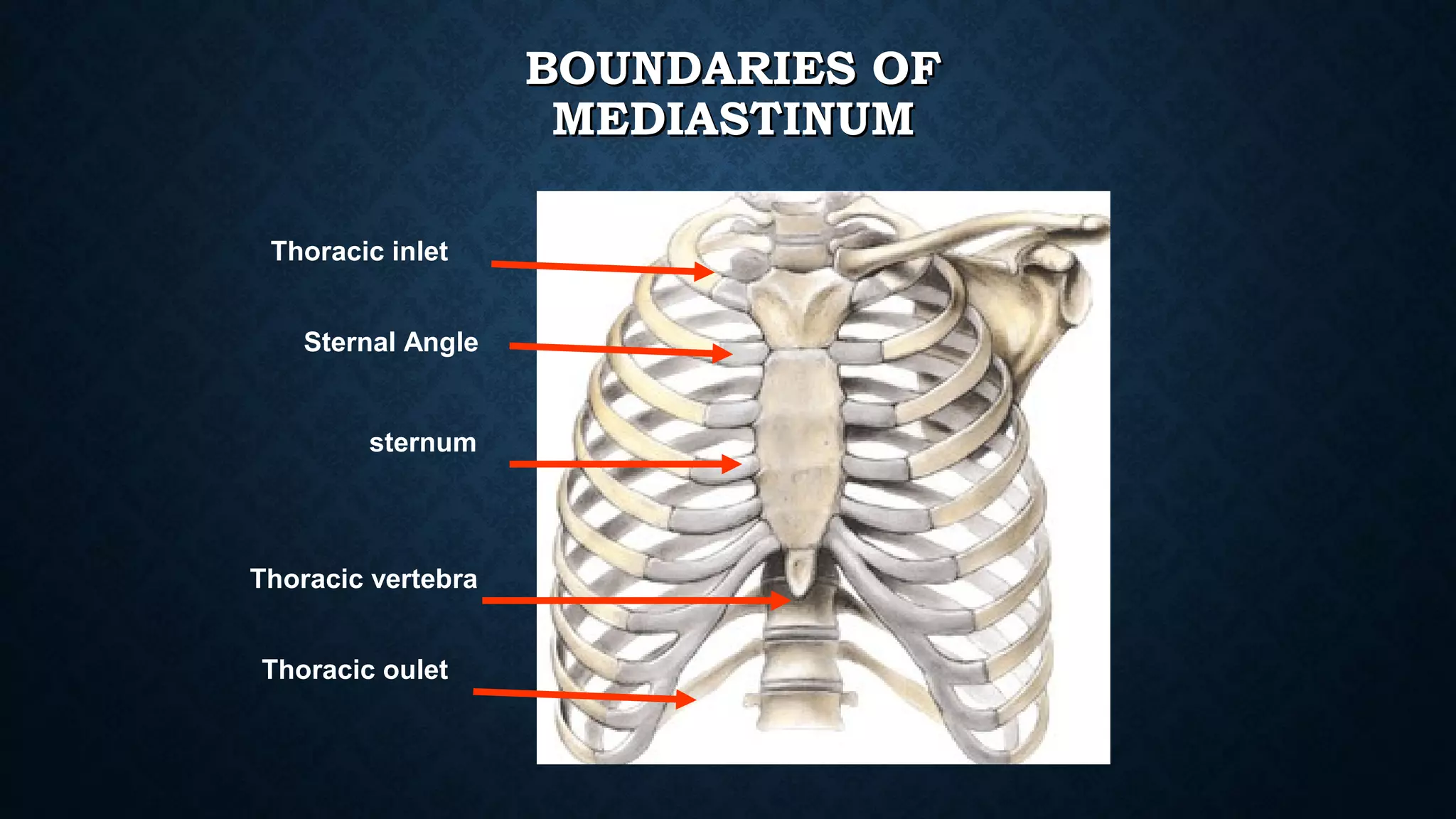
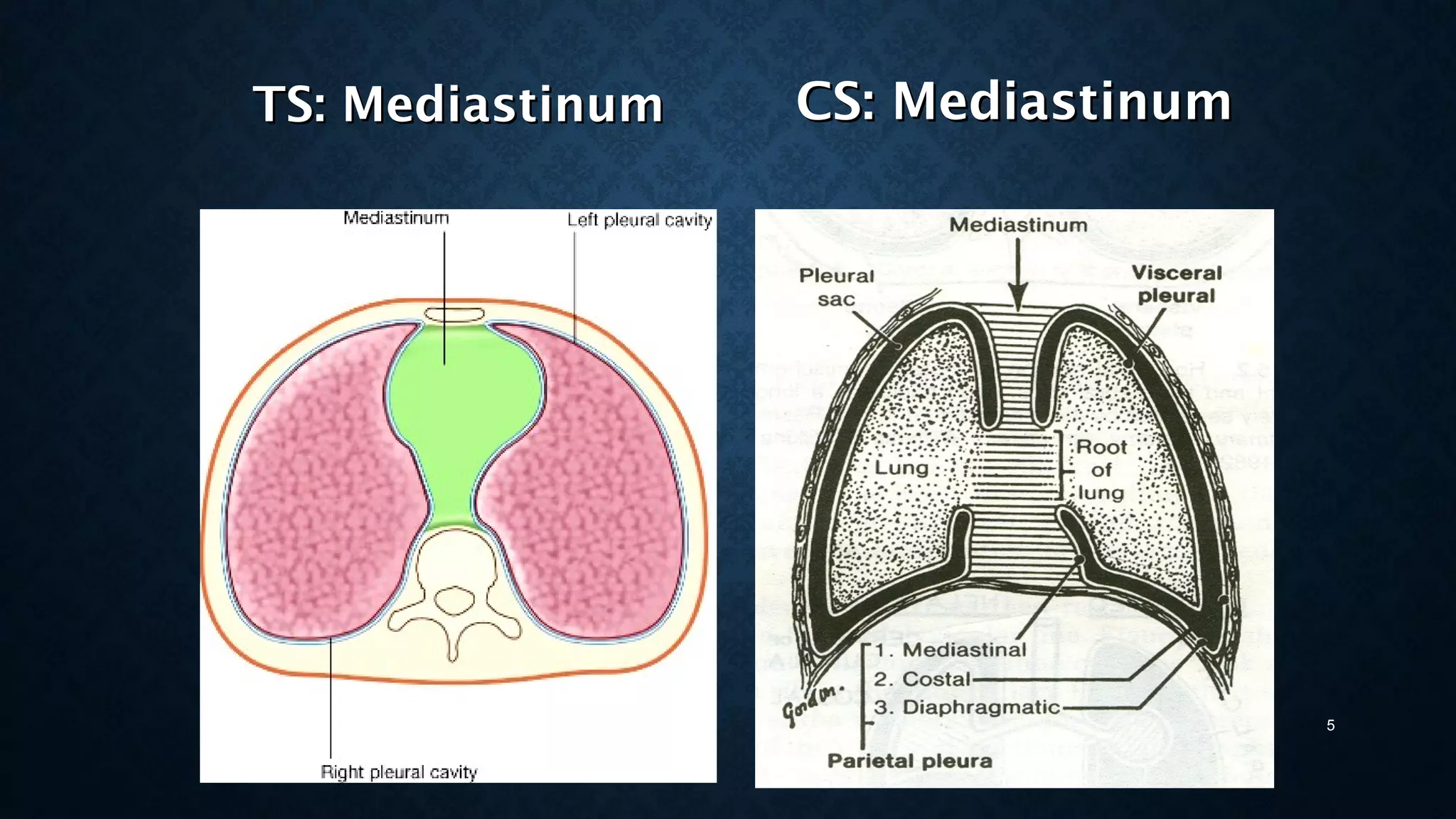
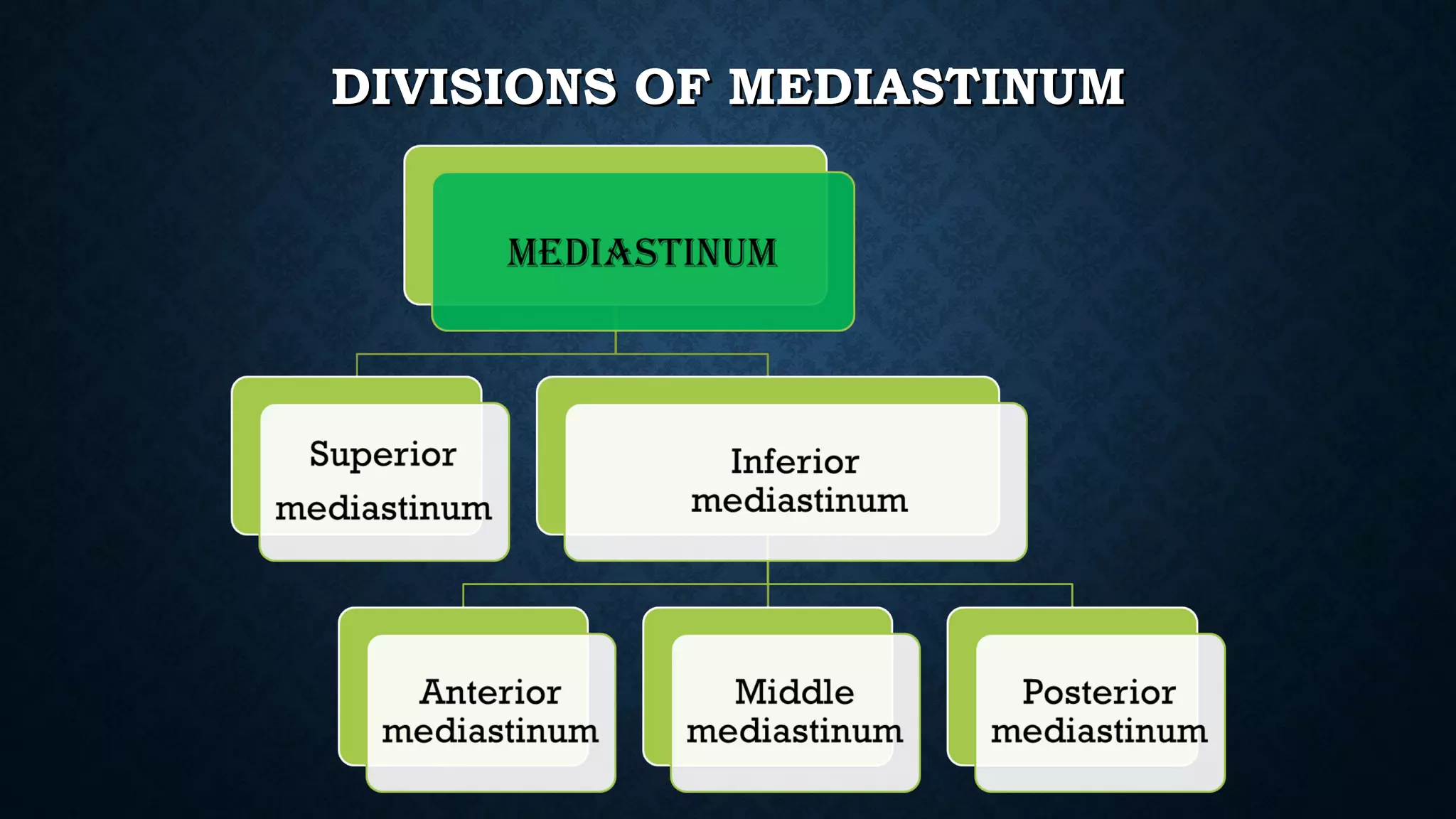
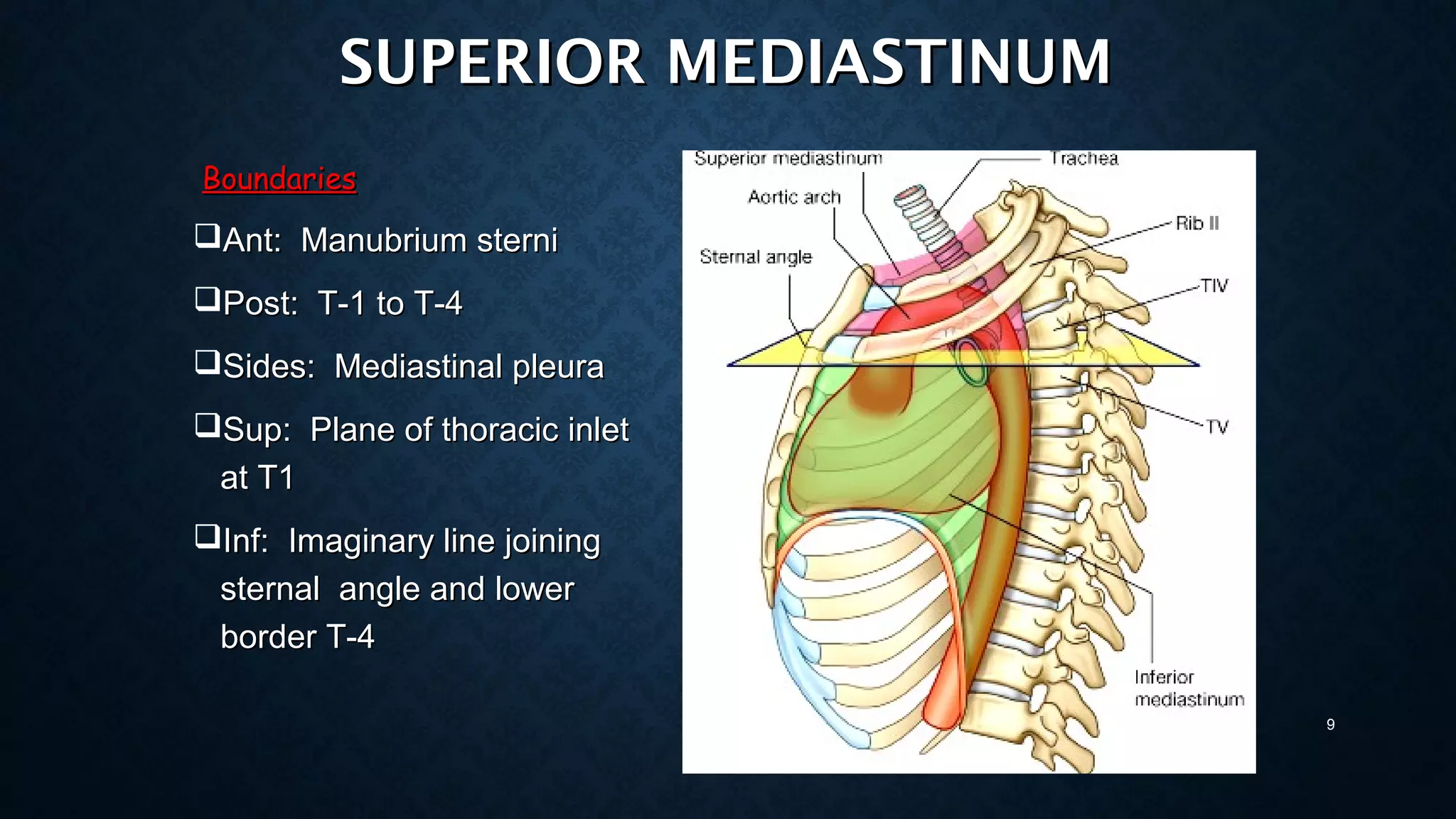
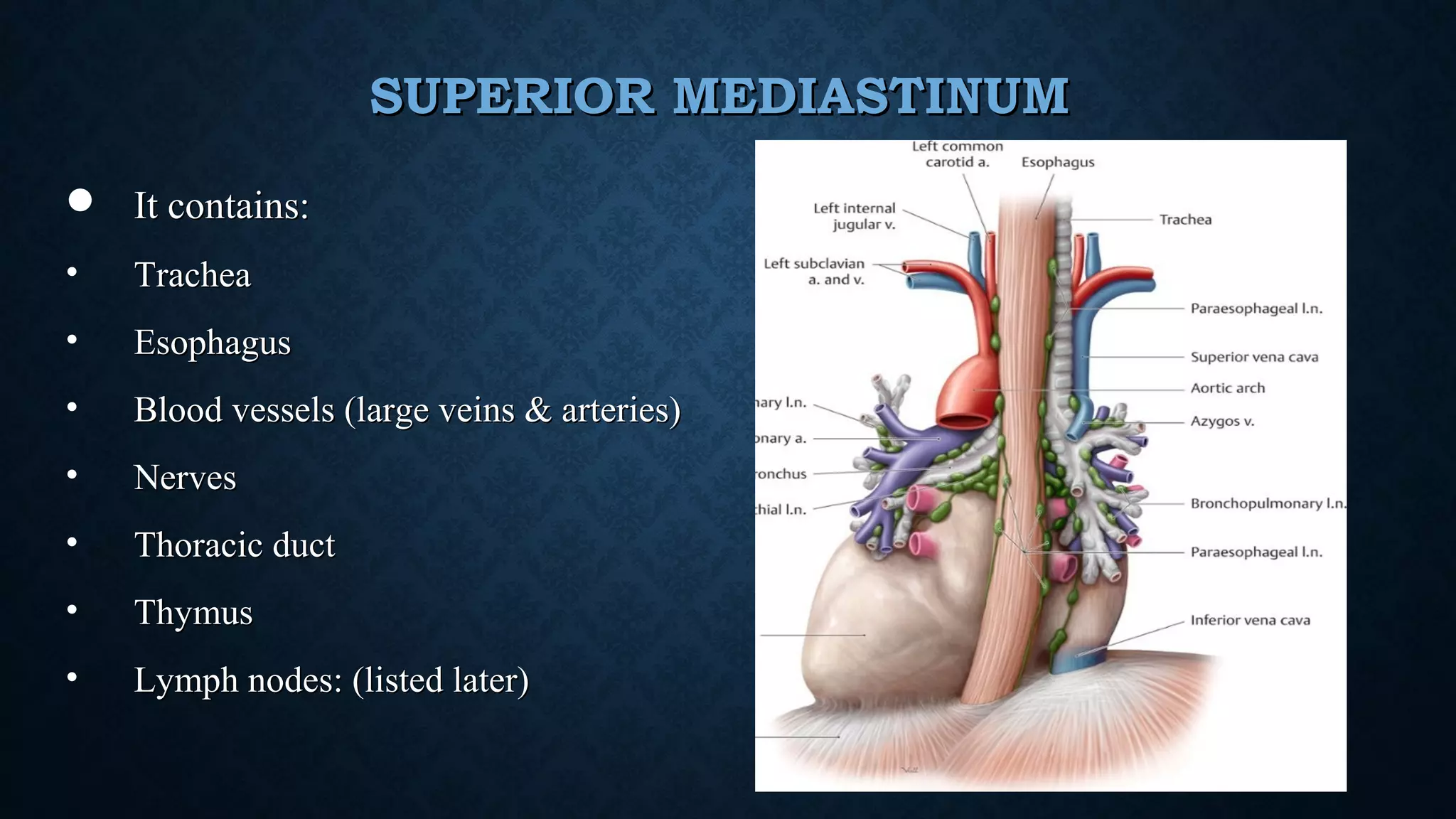
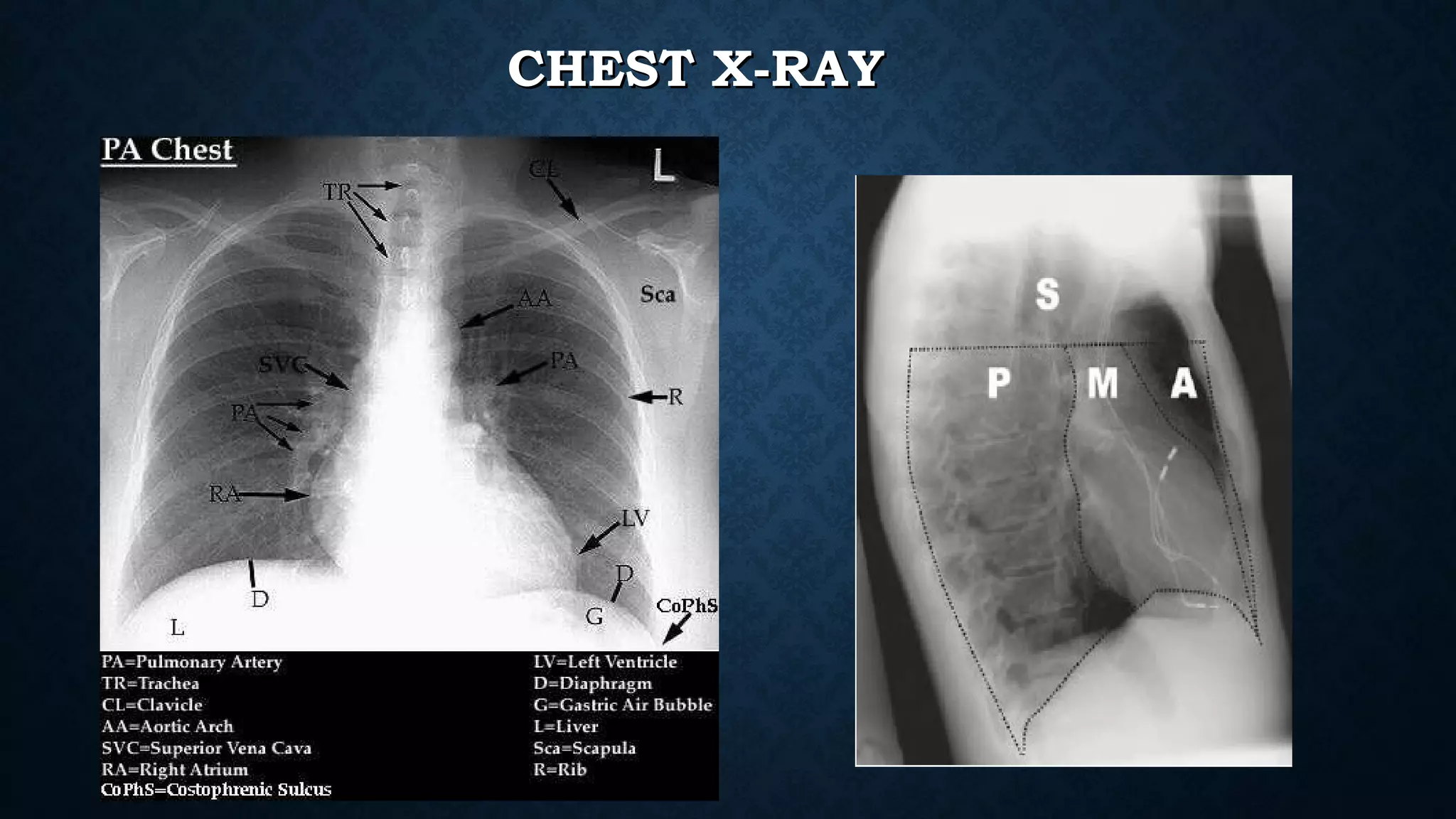
The document discusses the anatomy and divisions of the mediastinum. It is divided into superior and inferior mediastinum by an imaginary line passing through the sternal angle anteriorly and lower border of the 4th thoracic vertebra posteriorly. The inferior mediastinum is further divided into anterior, middle and posterior mediastinum. Each compartment contains different structures like blood vessels, nerves and lymph nodes. Common tumors in different mediastinal compartments are also mentioned. Radiological anatomy and signs to locate mediastinal masses are described along with epidemiology of mediastinal tumors.