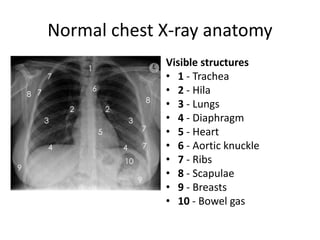
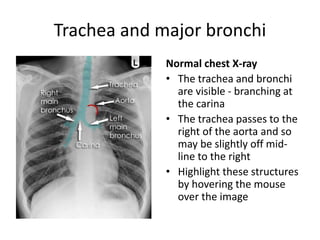
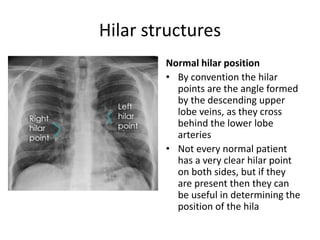
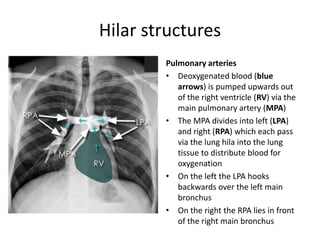
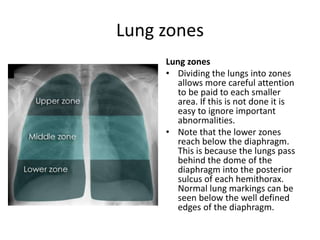
This document provides an overview of normal chest X-ray anatomy, including the 10 main visible structures and their typical appearance. It describes the trachea, hila, lungs, diaphragm, heart, bones, and other key points of assessment. The document emphasizes that a systematic approach is needed to evaluate each anatomical structure on every chest X-ray for abnormalities. Certain structures only become visible if abnormal and thorough assessment of the whole chest X-ray is important for accurate diagnosis.