Downloaded 95 times

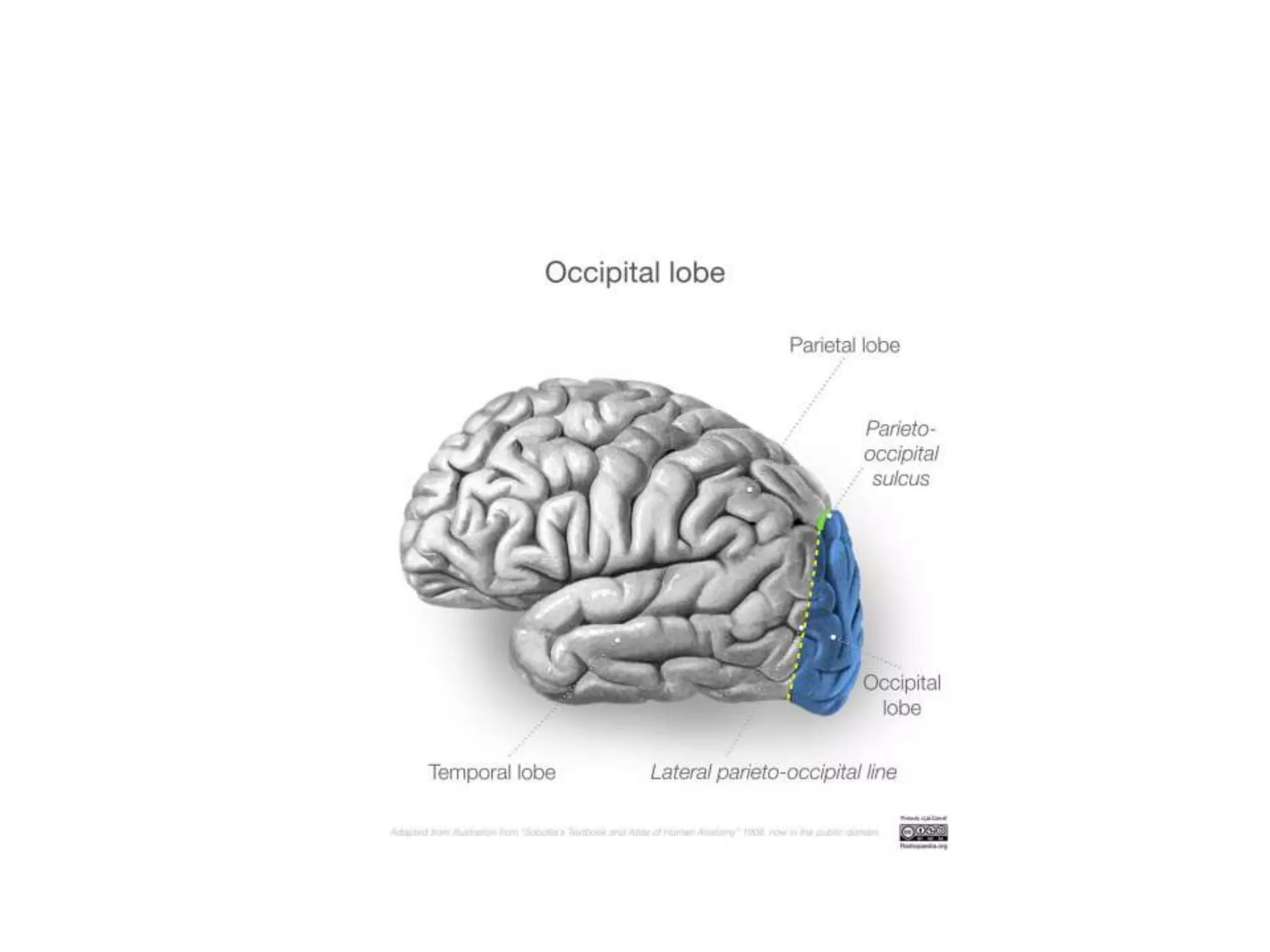




























































































This document discusses lesions in the occipital lobe and their effects. It covers topics such as field defects from lesions of the primary visual cortex, including homonymous hemianopia. It also discusses cortical blindness, Anton's syndrome, and other syndromes. Lesions of the ventral stream can cause visual agnosias like object agnosia and prosopagnosia. Disorders of the dorsal stream include Balint's syndrome and simultanagnosia. Various visual hallucinations and other positive visual phenomena are also covered. The document provides detailed information on the anatomical localization and clinical features of different visual disorders.