Downloaded 840 times

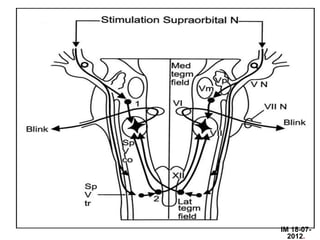
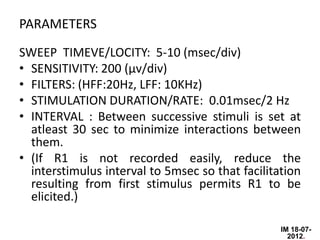
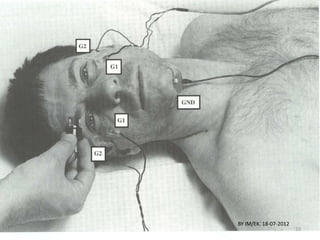
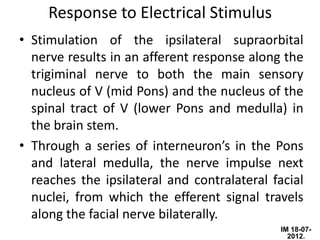
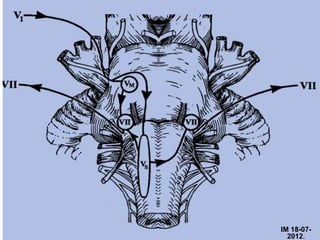
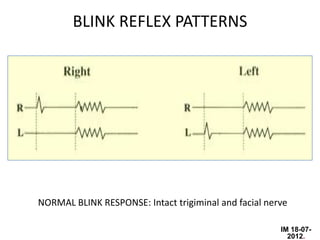
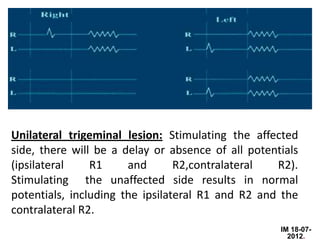
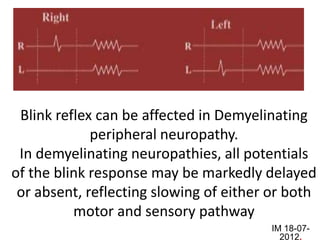
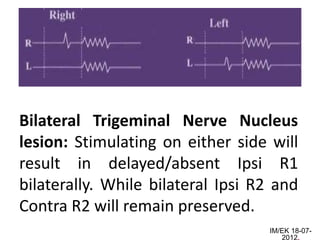

The document discusses the blink reflex, which evaluates the trigeminal and facial cranial nerves. Stimulation of the trigeminal nerve leads to contraction of the orbicularis oculi muscle mediated by the facial nerve. This produces two responses - an early R1 response localized to the stimulated side, and a later R2 response seen bilaterally. Analysis of blink reflex latencies can identify lesions along the afferent trigeminal or efferent facial nerve pathways or in the brainstem. The blink reflex is useful for evaluating various neurological conditions that may affect these cranial nerves or central pathways.



















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



