Downloaded 1,402 times
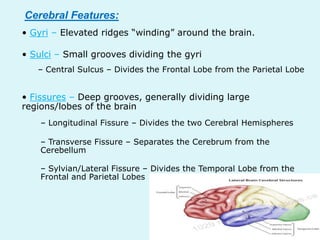
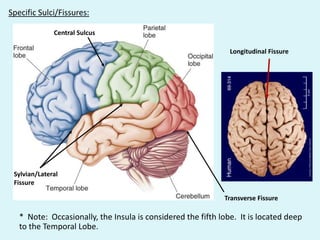
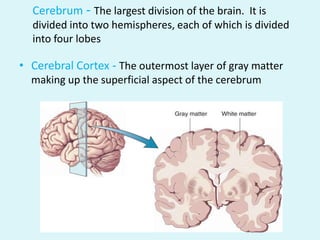
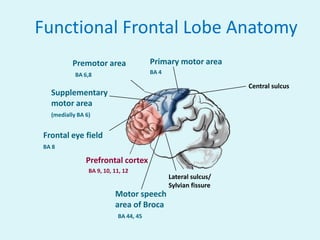
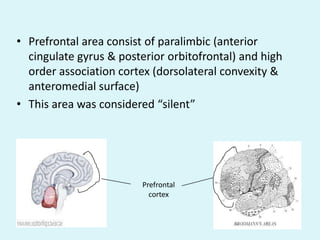
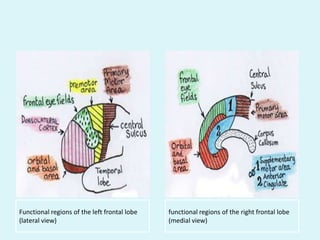
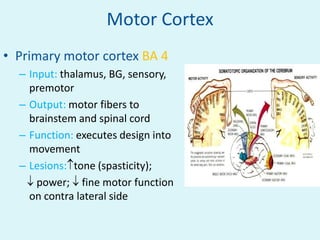
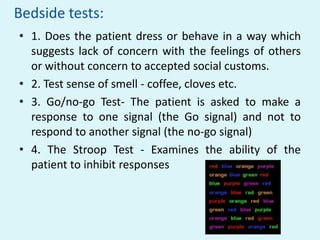
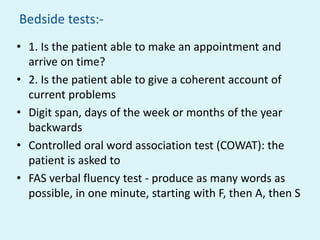
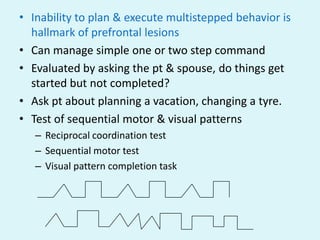
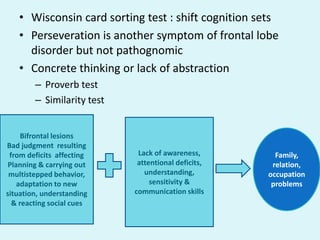
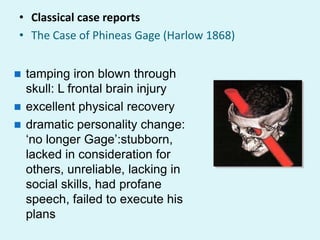


This document discusses the anatomy, functions, and clinical presentations of lesions involving the frontal lobe, including the motor cortex, prefrontal cortex, and their roles in executive function, social behavior, language, and more. Specific tests are described to evaluate functions like motor control, language, problem-solving, and emotional regulation that are mediated by the frontal lobe. A variety of clinical syndromes can result from frontal lobe lesions depending on the location and extent of the damage.























































































