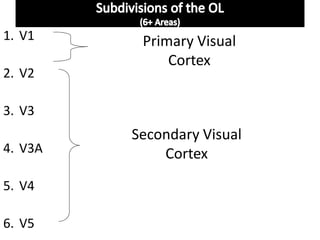
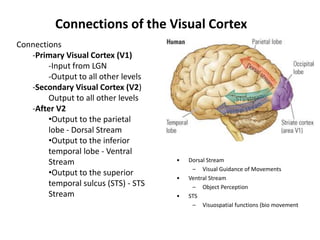
The occipital lobe is the visual processing center of the brain containing most of the visual cortex. It contains the primary visual cortex (V1) and several extrastriate areas involved in more complex visual tasks. Lesions can cause visual field defects, cortical blindness, visual agnosias or hallucinations depending on the location and extent of damage. Balint's syndrome and simultanagnosia involve bilateral lesions disrupting global visual perception while preserving local details.

























































































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































