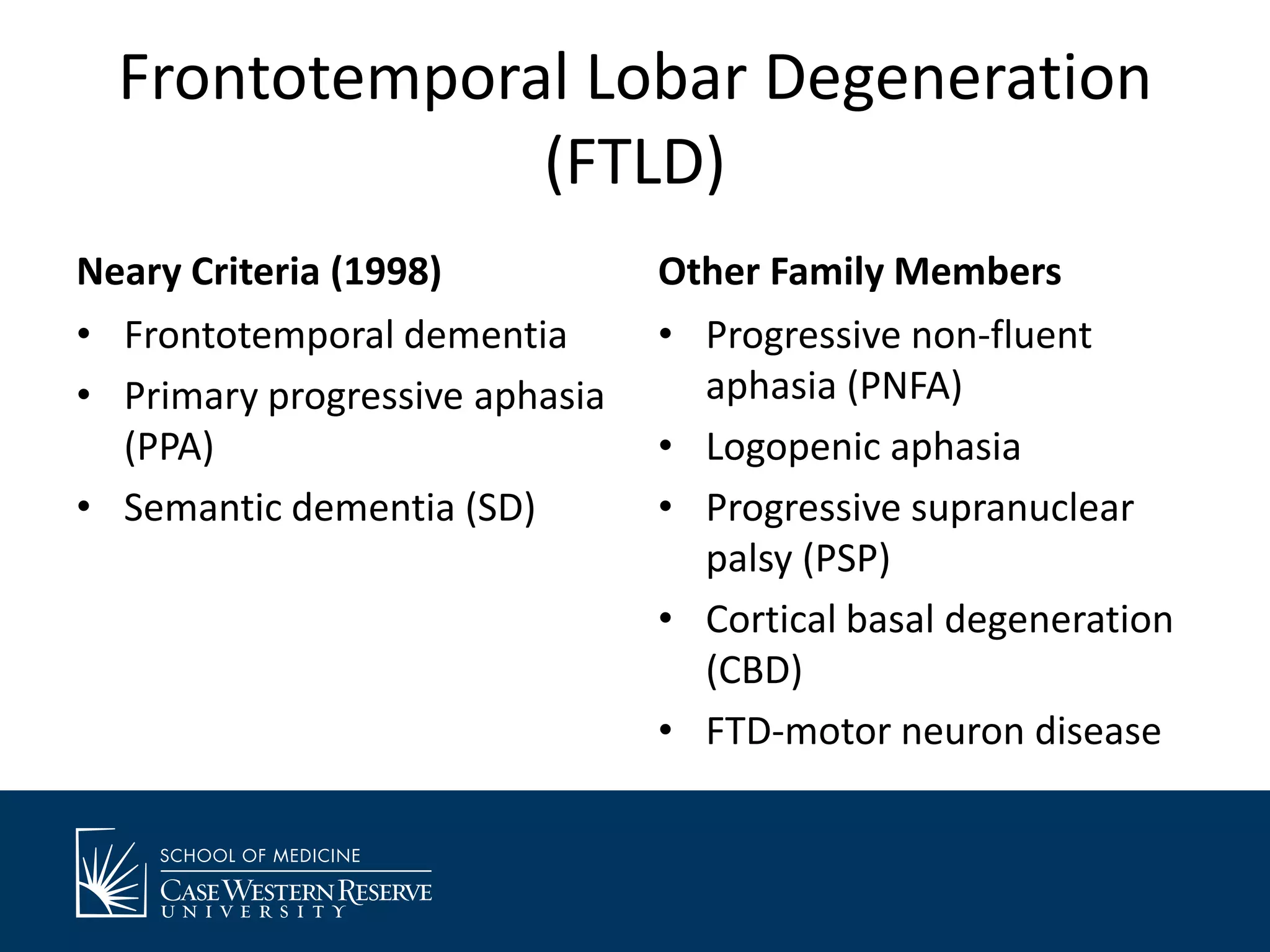
This document provides an overview of frontotemporal dementia (FTD) including its causes, clinical presentation, diagnosis, and management options. It discusses that FTD is caused by protein misfolding and accumulation in the brain. There are three main clinical variants - behavioral variant FTD, semantic dementia, and progressive nonfluent aphasia. Diagnosis involves ruling out other causes and may include brain imaging. Treatment focuses on managing symptoms but medications have limited effectiveness. Caregiver burden can be high due to patient behaviors, so support groups are recommended.