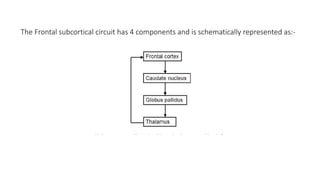
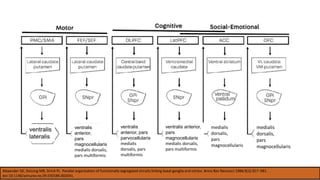
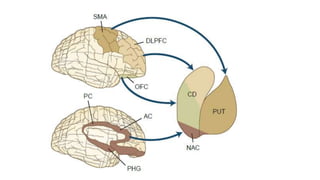
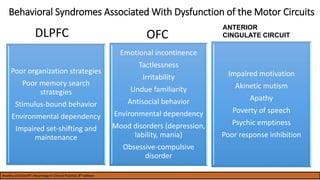
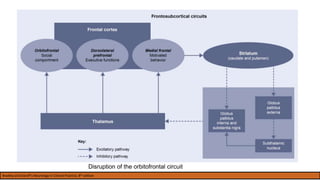
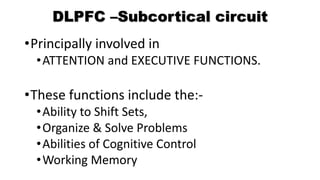
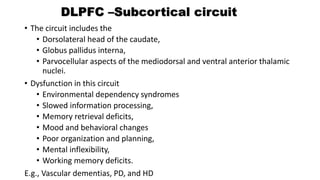
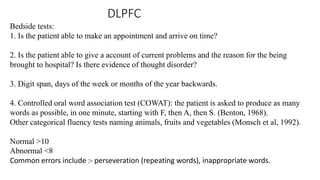
The document discusses frontal subcortical circuits and their assessment. It describes the five main frontal-subcortical circuits, including the motor circuit, oculomotor circuit, dorsolateral prefrontal circuit, anterior cingulate circuit, and orbitofrontal circuit. It then examines each circuit in more detail, outlining their anatomical components and behavioral syndromes associated with dysfunction. A number of bedside assessment tests are also presented to help evaluate specific circuits.








































![Frontal Lobe Syndromes [2014]](https://cdn.slidesharecdn.com/ss_thumbnails/fls2014zo-170704023944-thumbnail.jpg?width=640&height=640&fit=bounds)













![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































