Downloaded 68 times




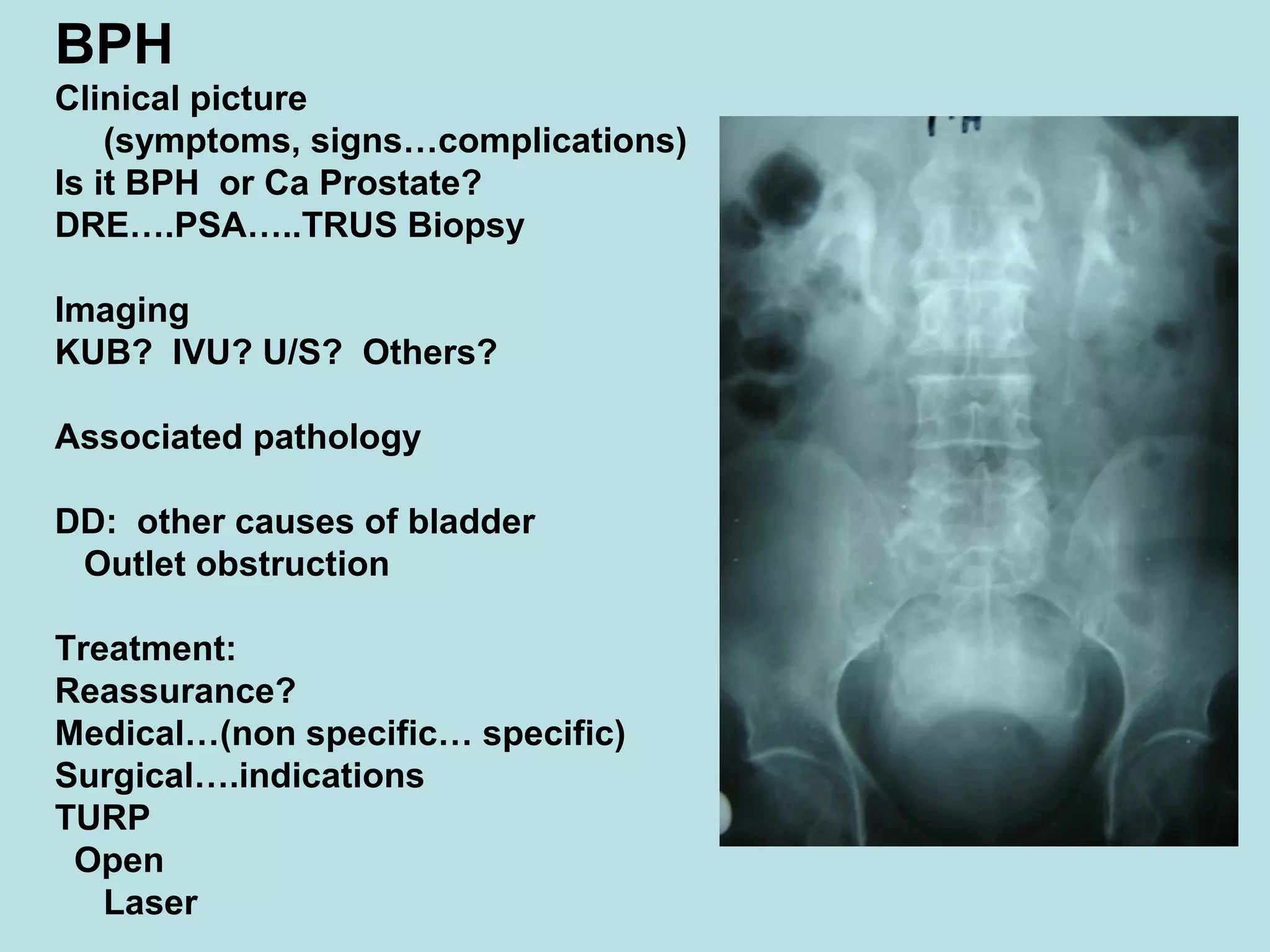








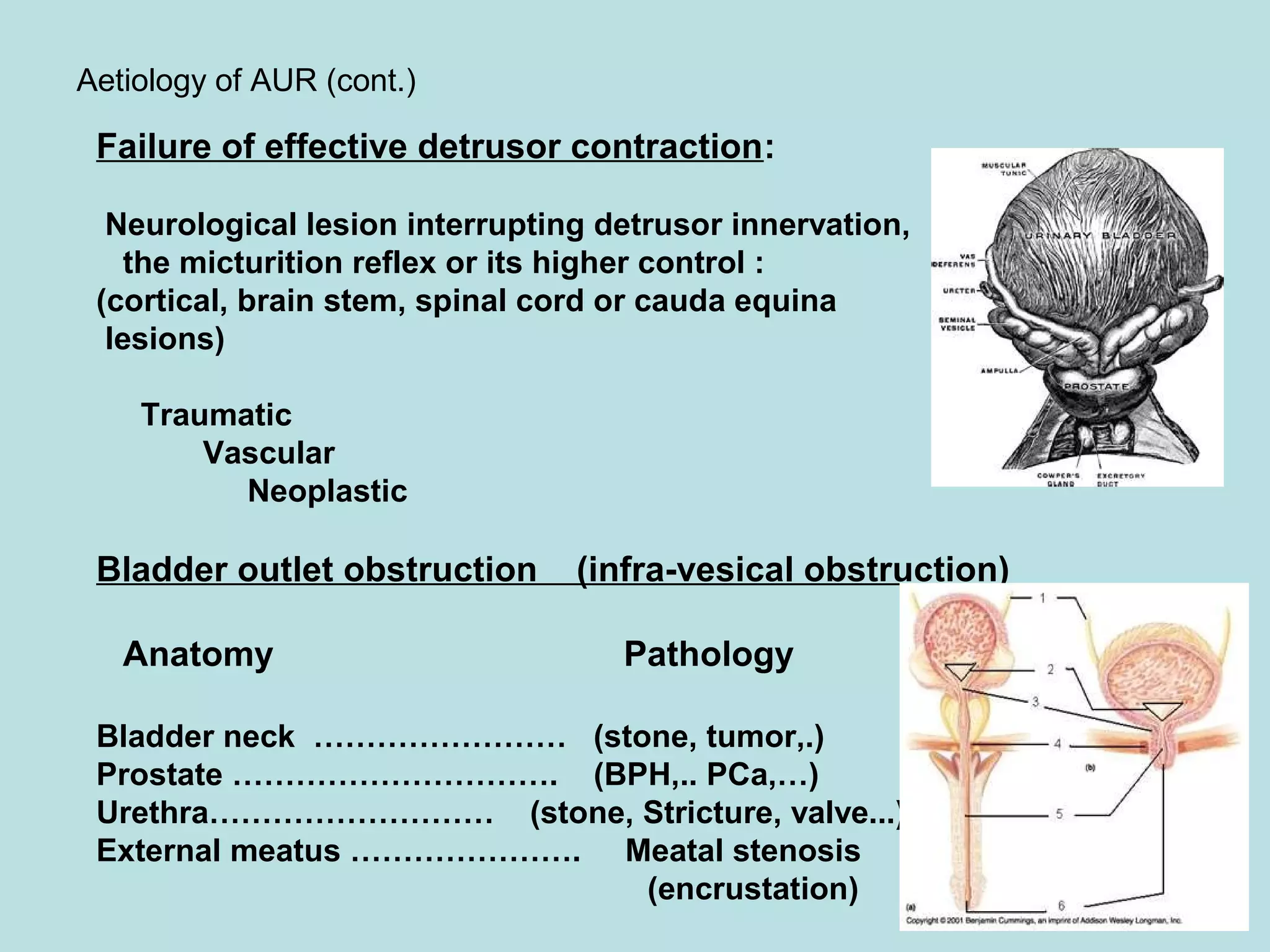













Acute urinary retention (AUR) is the inability to void despite a full bladder. It can be caused by failure of detrusor contraction or bladder outlet obstruction. Diagnosis involves confirmation of a full bladder on exam and insertion of a urethral catheter. Immediate treatment is catheterization to evacuate the bladder. Further evaluation is then done to identify the underlying cause and provide definitive treatment.



































![Benign Prostatic Hyperplasia BPH [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/bphedmond-140716213908-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)







































































