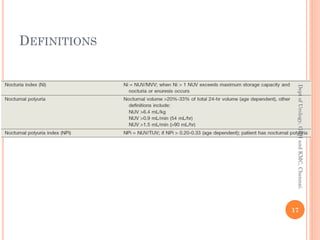
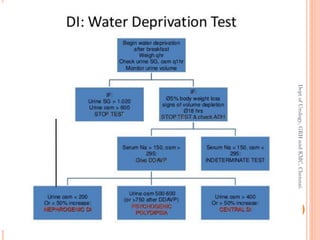
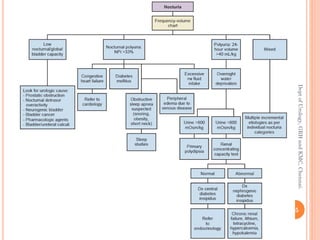
This document discusses nocturia (waking at night to urinate) and its causes and management. It defines nocturia and provides the international continence society definition. It discusses the prevalence of nocturia increasing with age for both men and women. Nocturia can be caused by nocturnal polyuria (excess night urine production), diminished bladder capacity, or global polyuria (excess 24-hour urine production). Evaluation involves assessing urine volume and frequency. Management depends on the underlying cause and may include medications, surgery, behavioral changes, and treating any contributing medical conditions.