Downloaded 421 times

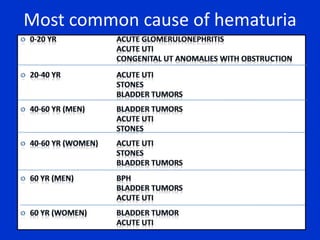
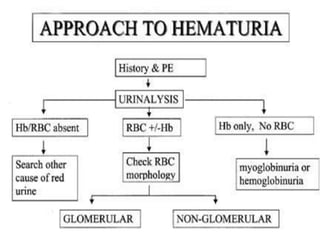
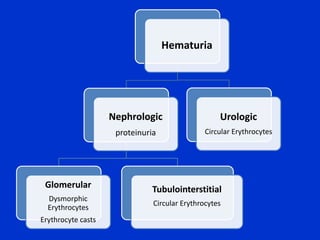
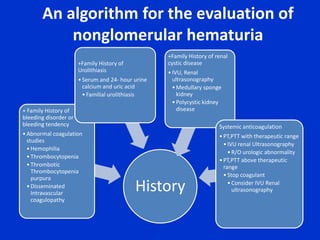
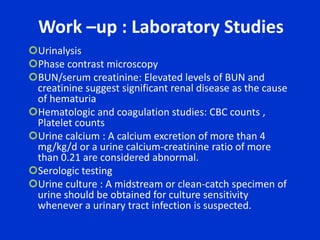
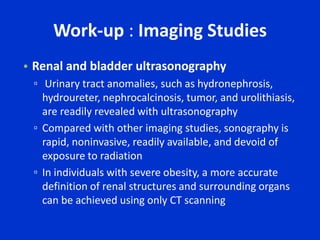
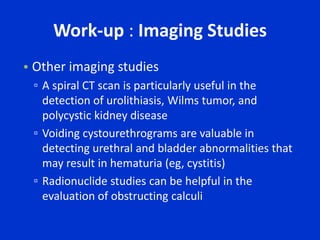
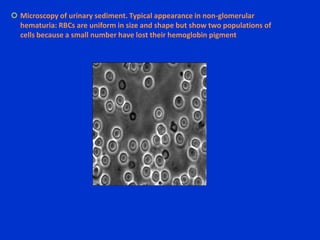
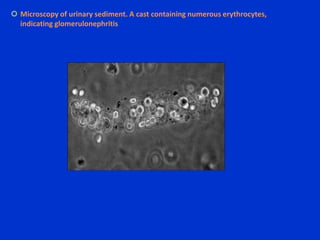
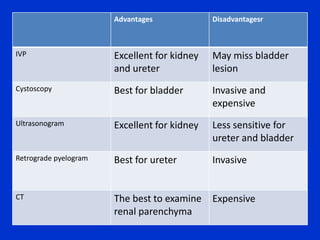
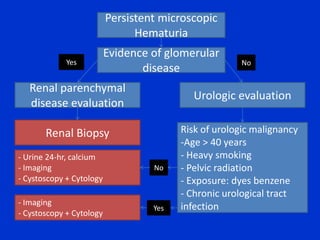
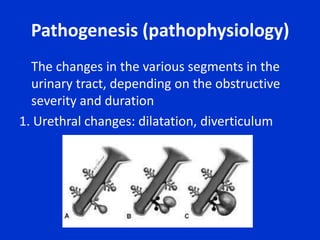
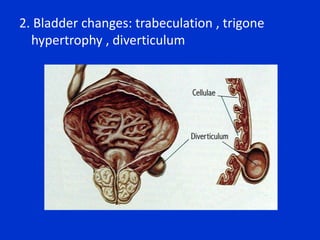
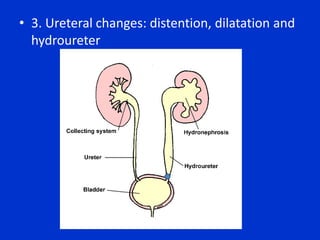
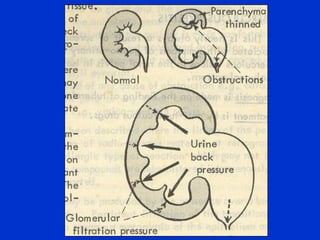
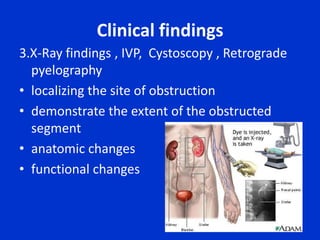


This document discusses hematuria (blood in the urine) and obstructive uropathy (blockage of urine flow in the urinary tract). It covers evaluating hematuria through urinalysis, imaging tests, and cystoscopy. Common causes of hematuria include infections, stones, tumors, and glomerulonephritis. Obstructive uropathy can be congenital or acquired and cause changes to the urethra, bladder, ureters, and kidneys over time. Relieving the obstruction through surgery, stents, or nephrostomy is the main treatment approach.























































































