Downloaded 173 times




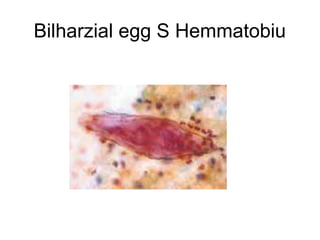

1. Bladder tumors can be epithelial like papillomas or carcinomas, or mesenchymal like leiomyomas or sarcomas. 2. In Egypt, bladder cancer is most common in males, with a male to female ratio of 3:1 and peak incidence between ages 30-50 due to bilharziasis. 3. Bilharzial bladder carcinoma presents at a younger age, with higher male predominance and more squamous cell carcinoma histology compared to non-bilharzial bladder cancer.






































![Bladder Cancer NMIBC [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/non-muscleinvasivebladdertumoredmond-140716212950-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)
















































