Downloaded 324 times
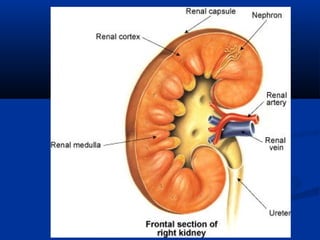
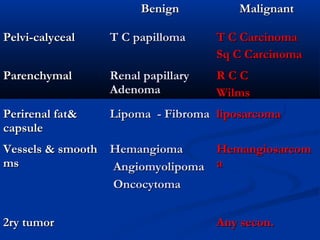
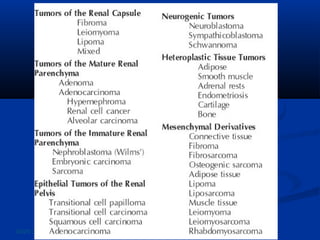
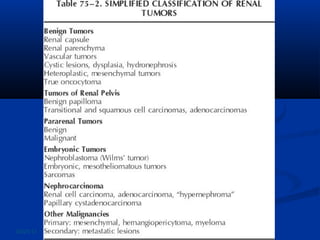
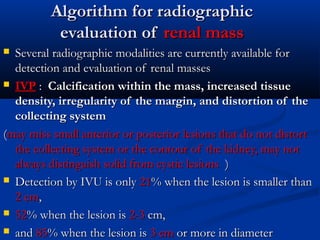



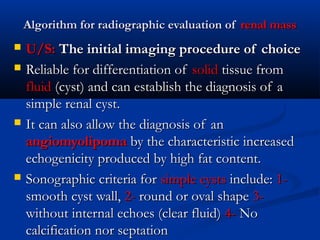
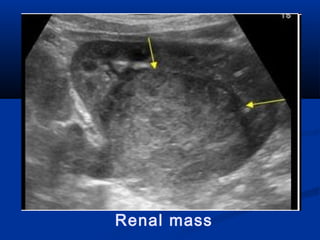
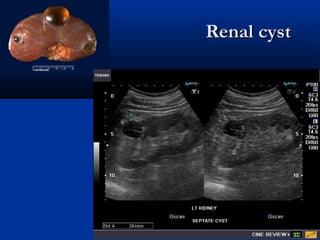
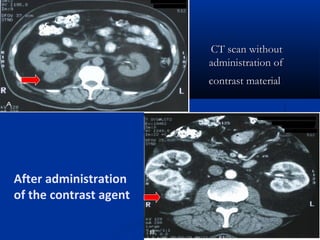
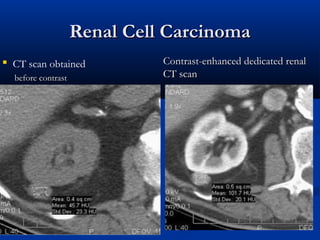
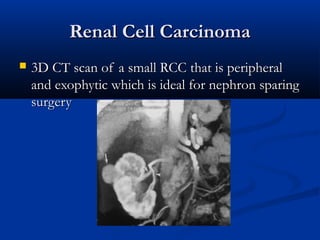
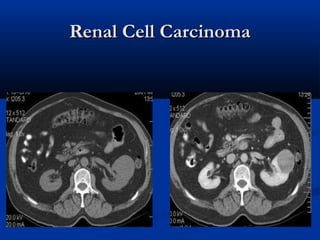
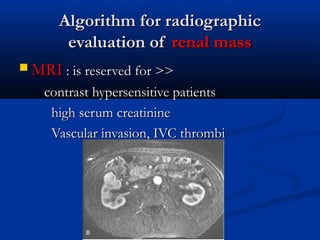




Renal masses can be benign or malignant tumors arising from the renal parenchyma or other structures. Computed tomography (CT) scan is the most important test to characterize renal masses and distinguish solid enhancing lesions, which are often renal cell carcinomas (RCC), from simple cysts. MRI may be used if the patient has contrast allergy or renal insufficiency. Biopsy has limited use and is mainly to differentiate RCC from metastatic disease or infection. Small benign tumors like adenomas are considered for resection due to difficulty differentiating them from RCC radiographically.











































































































