Downloaded 243 times


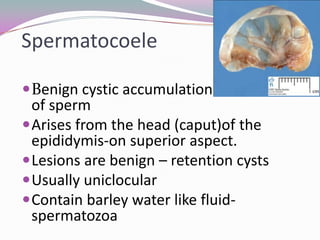















Spermatocele is a benign cystic accumulation of sperm that arises from the head of the epididymis. It typically presents as an asymptomatic mobile swelling near the testicle. Ultrasound shows a hypoechoic cystic lesion connected to the epididymis. Treatment involves observation for small asymptomatic cases or spermatocelectomy via scrotal surgery to remove the cyst. Sclerotherapy is sometimes used as an alternative but has a higher recurrence rate.






































































































