Downloaded 193 times
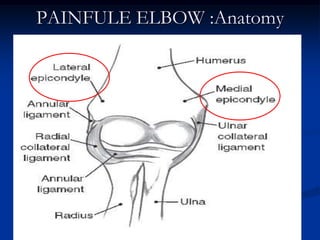
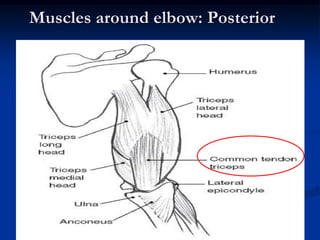
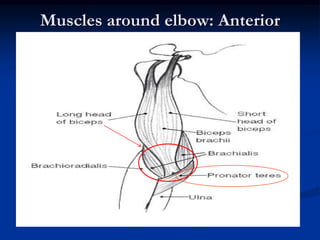
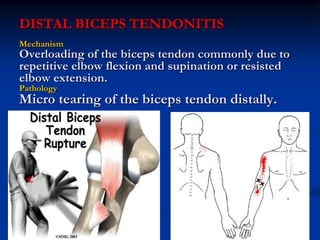
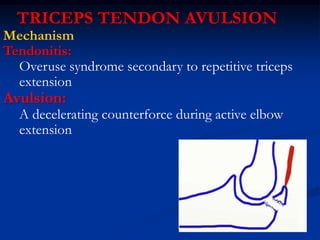

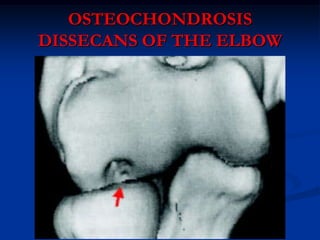

This document discusses various causes of elbow pain, including generalized causes like arthritis, infections, and trauma, as well as more localized causes. Some common localized causes covered include medial and lateral epicondylitis (golfer's and tennis elbow), olecranon bursitis, elbow dislocations, distal biceps tendonitis, triceps tendon avulsions, valgus extension overload syndrome, ulnar and radial collateral ligament sprains, pronator syndrome, cubital tunnel syndrome, osteochondrosis dissescans of the elbow, and fractures of the humerus, distal humerus, radial head, and olecranon. Evaluation and treatment approaches including conservative and surgical options are provided































































































