
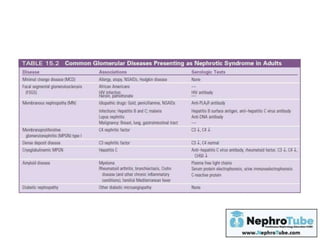
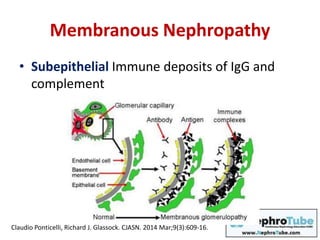
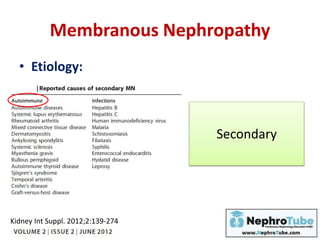
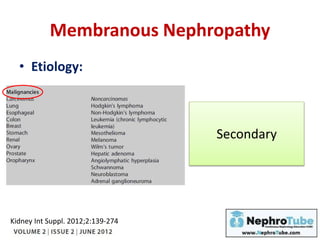
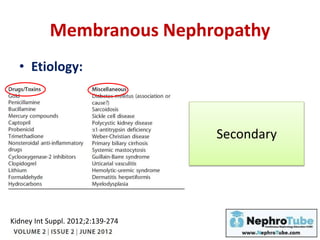
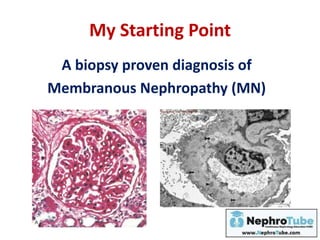

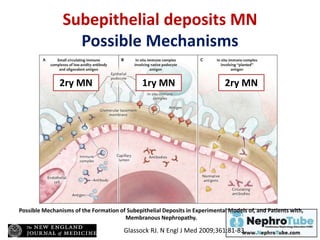
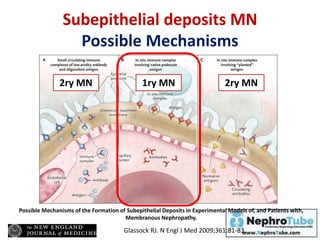
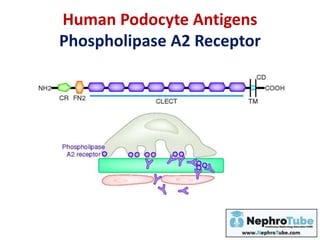

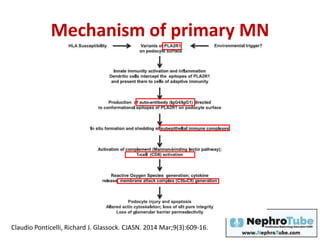
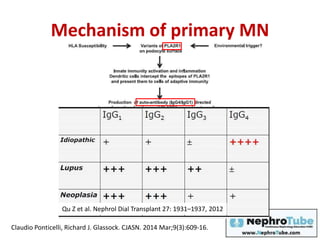
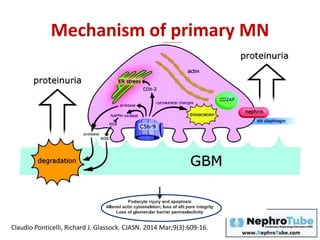
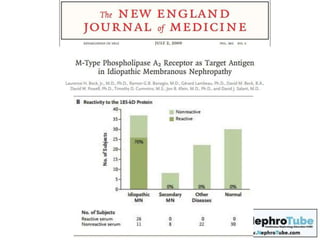
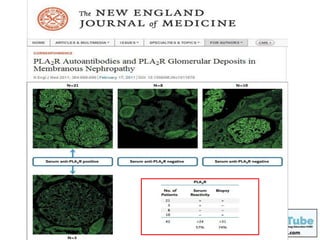
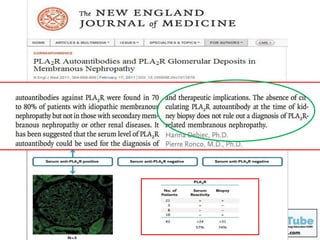
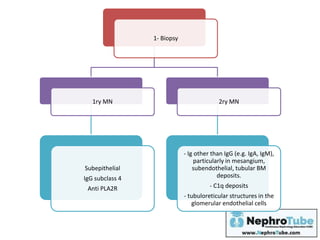
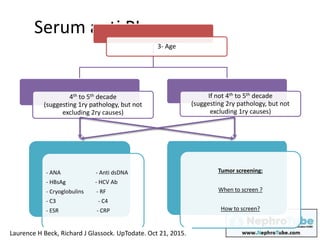
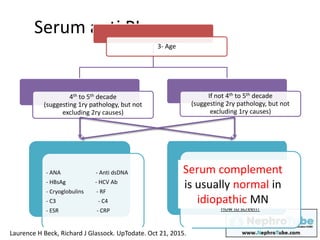
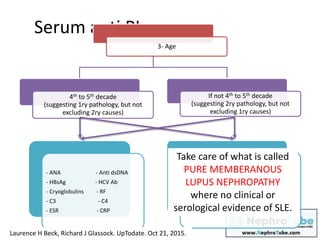
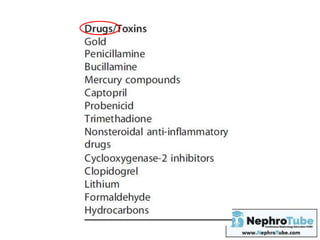

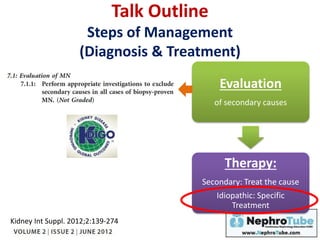
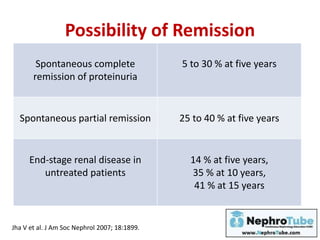
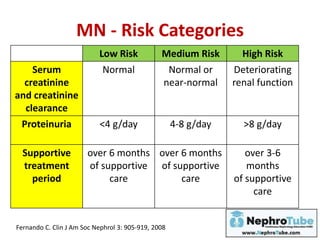
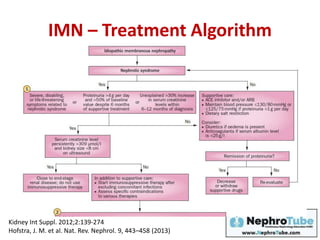
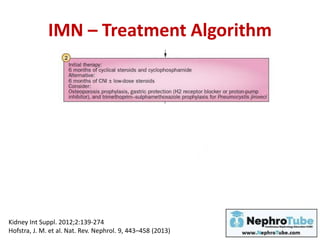
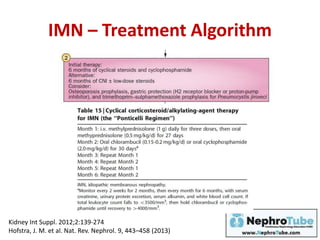
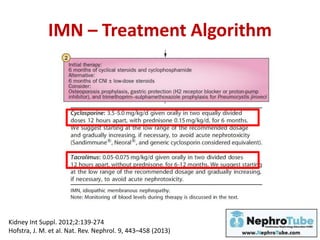
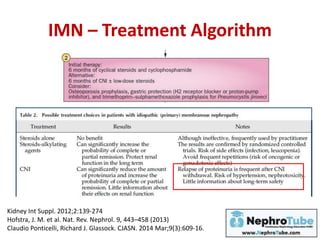
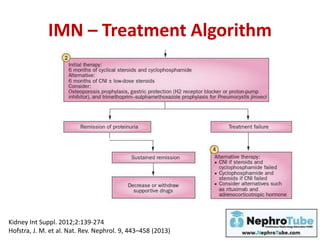
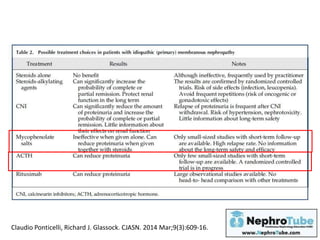
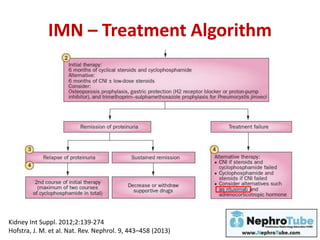
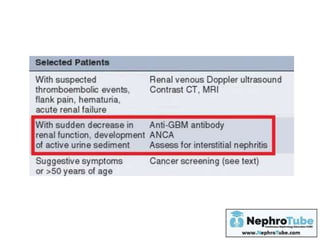
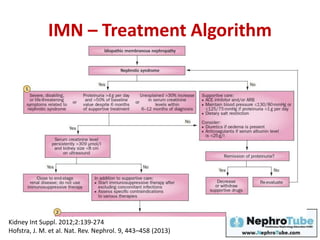
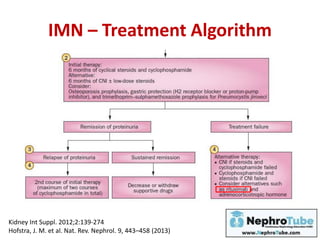
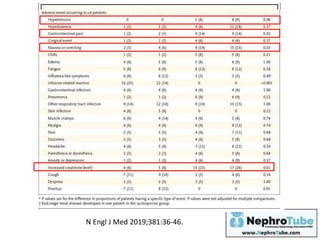
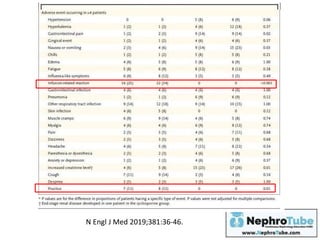
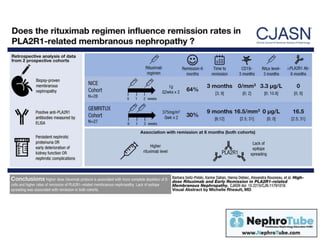
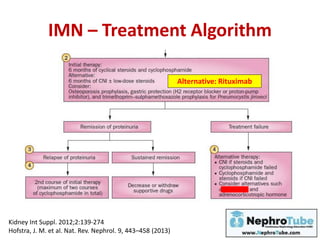


The document discusses membranous nephropathy (MN), a glomerular disease characterized by nephrotic syndrome and subepithelial immune deposits. Key features of the disease's diagnosis, treatment strategies, and potential remission rates are outlined, highlighting both primary and secondary causes. It also emphasizes the significance of anti-PLA2R antibodies in relation to MN and provides an overview of management approaches, including therapy options based on risk categories.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


