Downloaded 124 times
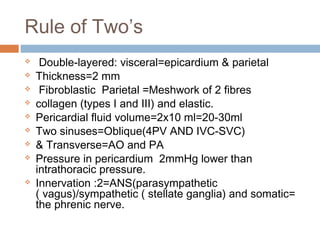
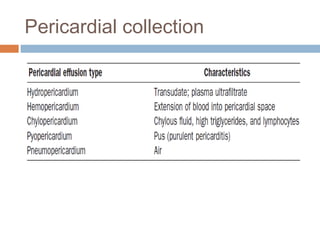
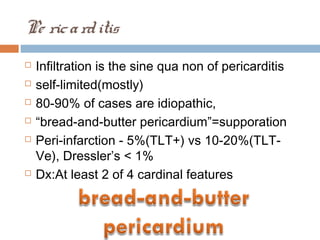
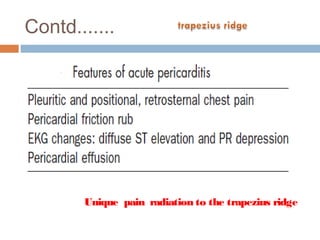

The document discusses the anatomy, physiology, embryology, and clinical significance of the pericardium, emphasizing its double-layered structure and the role of pericardial fluid in facilitating heart movement. It covers pathological conditions like pericarditis and pericardial effusion, their diagnosis, and treatment options, and highlights the hemodynamic consequences related to heart function. The document also mentions various congenital defects and the significance of pressures in the pericardial space impacting cardiac dynamics.








































































































