Downloaded 402 times
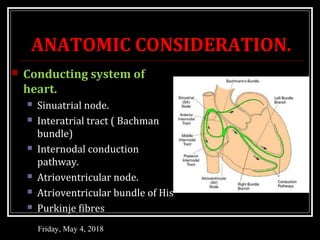
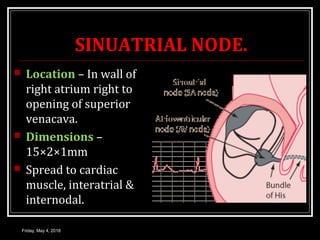
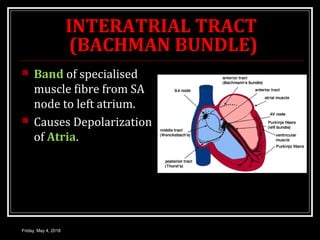
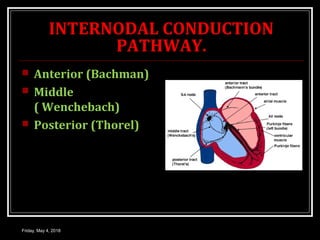

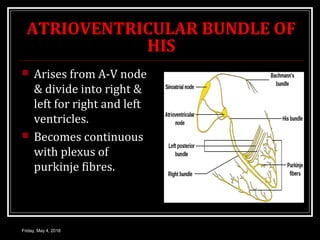
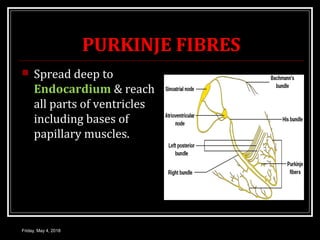
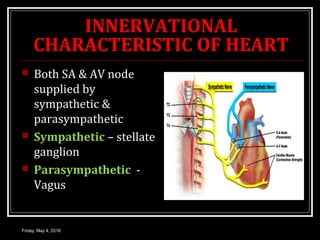
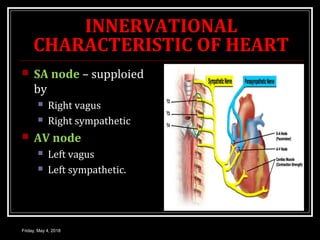
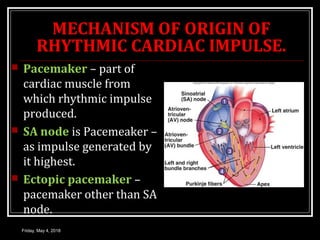
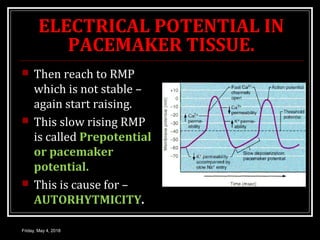
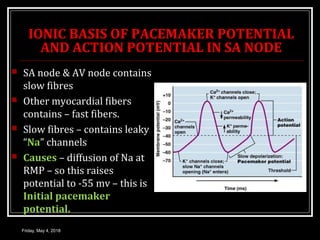
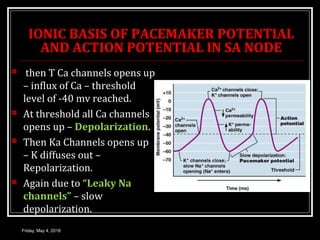
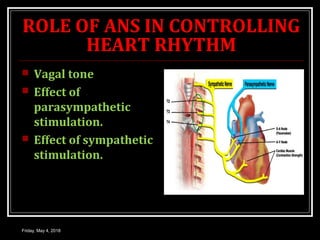
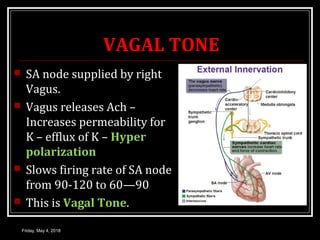
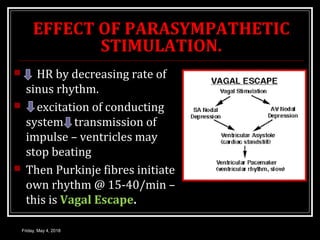
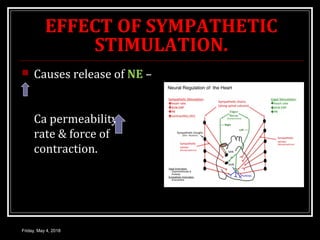
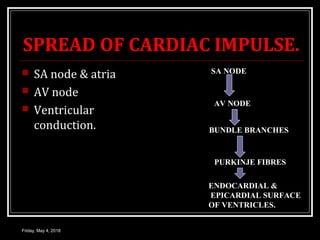


This document discusses the conduction system of the heart, including the sinoatrial node, atrioventricular node, bundle of His, and Purkinje fibers. It describes how these structures work together to generate and coordinate the heartbeat. The sinoatrial node initiates impulses at a rate of 70-80 beats per minute. Impulses then spread to the atria and through the atrioventricular node to the ventricles via the bundle of His and Purkinje fibers. The autonomic nervous system can influence heart rate through the release of acetylcholine or norepinephrine on the sinoatrial and atrioventricular nodes.