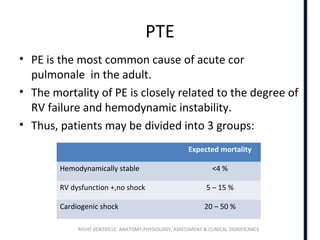
Downloaded 310 times
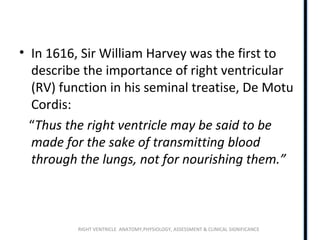
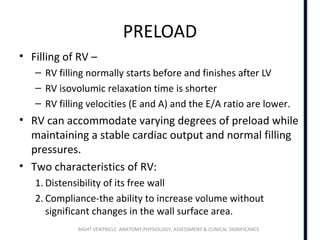
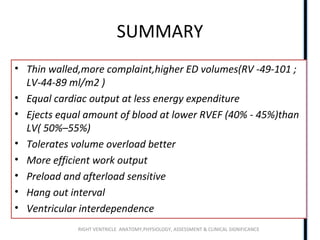
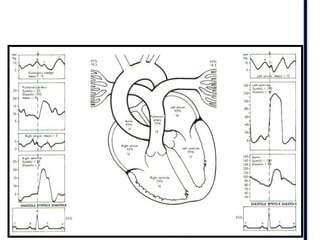
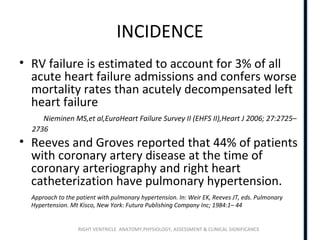
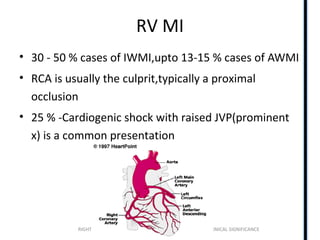
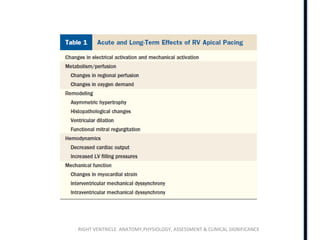
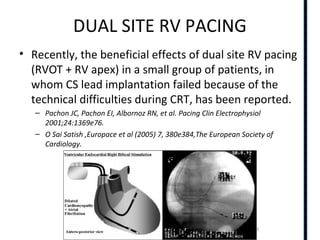
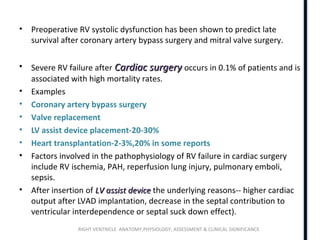
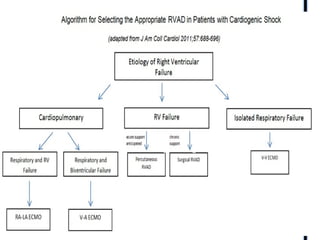
![• Maximal RV elastance
better reflects RV
contractility than does
the end-systolic
elastance.
• The normal maximal RV
elastance is 1.3 +/-0.84
mm Hg/mL(study by
Dell’Italia and Walsh)
[LV -5.48 +/-1.23]](https://image.slidesharecdn.com/rightventricle2003-180722063343/85/Right-ventricle-RV-anatomy-and-functions-21-320.jpg)

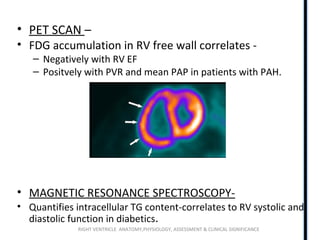
![RIGHT VENTRICLE ANATOMY,PHYSIOLOGY, ASSESSMENT & CLINICAL SIGNIFICANCE
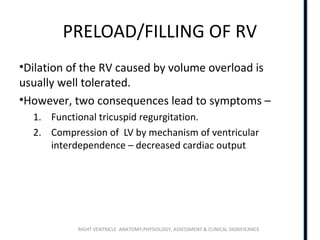
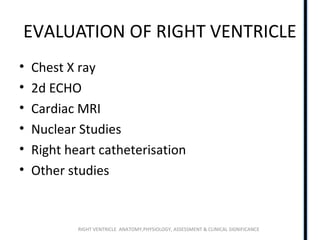
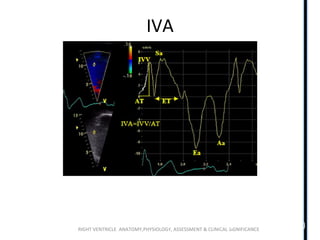
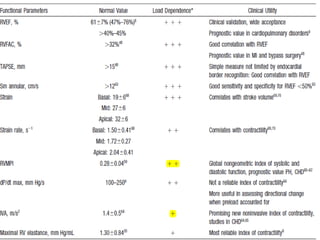
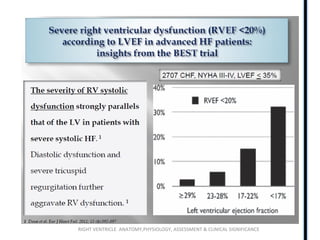
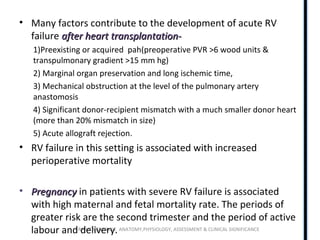
RIMP
• The MPI, also known as the RIMP or Tei index, is a global
estimate of both systolic and diastolic function of the
right ventricle
• The MPI is defined as the ratio of isovolumic time divided
by ET, or [(IVRT + IVCT)/ET]
• Normal right-sided MPI = 0.28+/-0.04
• Yoshifuku and colleaguesdescribed pseudonormalized values in
acute and severe RV myocardial infarction, which can probably be
explained by a decrease in isovolumic contraction time associated
with an acute increase in RV diastolic pressure](https://image.slidesharecdn.com/rightventricle2003-180722063343/85/Right-ventricle-RV-anatomy-and-functions-44-320.jpg)





![RIGHT VENTRICLE ANATOMY,PHYSIOLOGY, ASSESSMENT & CLINICAL SIGNIFICANCE
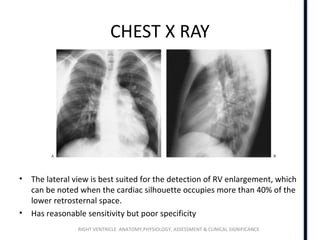
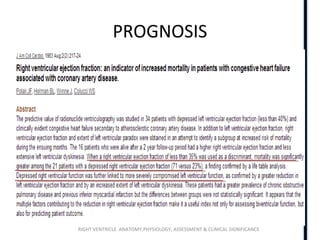
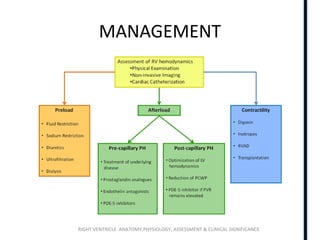
LONG TERM PROGNOSIS
• In those who survive RVMI, the long-term prognosis is primarily
determined by the extent of left ventricular involvement.
• Nearly complete recovery of RV function has been shown to occur in 62 to
82 percent of patients within the first few months
– Frequency and significance of right ventricular dysfunction during inferior wall left ventricular myocardial infarction treated with
thrombolytic therapy (results from the thrombolysis in myocardial infarction [TIMI]II trial). The TIMI Research Group,Am J
Cardiol. 1993;71(13):1148
– Prognostic significance of persistent right ventricular dysfunction as assessed by radionuclide angiocardiography in patients with
inferior wall acute myocardial infarction,Am J Cardiol. 2000;85(8):939
• Chronic right heart failure attributable only to right ventricular infarction
is rare,even in those without successful reperfusion
• Over the long term, a persistent reduction in right ventricular function
appears to be associated with a worse long-term prognosis
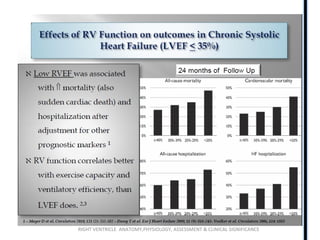
• During a mean follow-up of 17 months, patients with an RVEF <40 percent
had a significantly higher mortality compared to those with an RVEF >40
percent (adjusted hazard ratio 2.9).](https://image.slidesharecdn.com/rightventricle2003-180722063343/85/Right-ventricle-RV-anatomy-and-functions-110-320.jpg)



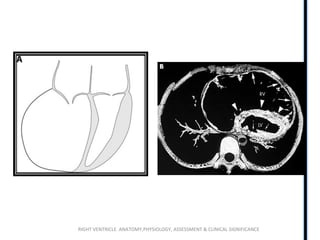








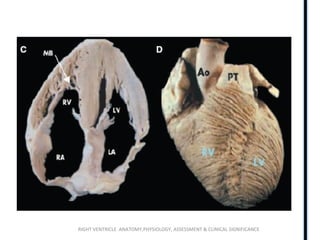
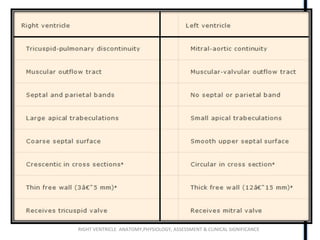
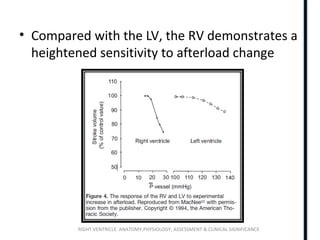
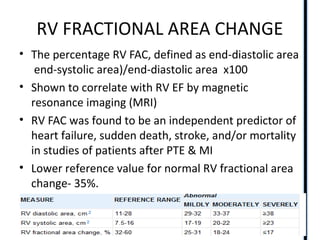
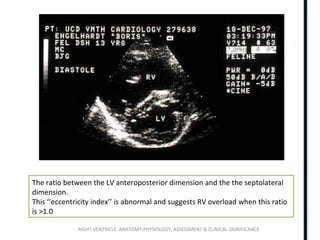
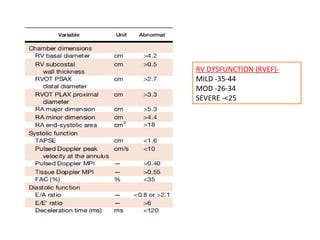
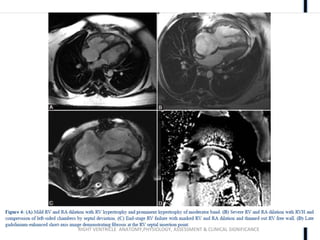
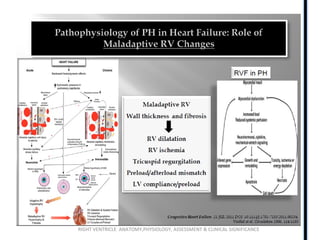
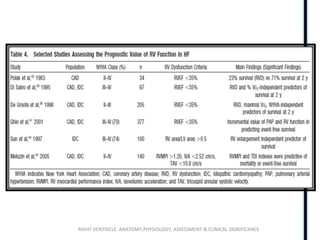
The document discusses the anatomy, physiology, assessment, and clinical significance of the right ventricle. Some key points include: - The right ventricle is crescent-shaped and thinner-walled than the left ventricle. It has a higher preload and is more sensitive to changes in afterload. - Assessment of the right ventricle includes echocardiography measures like fractional area change, TAPSE, and septal position. Hemodynamic measures include pulmonary artery pressures, pulmonary vascular resistance, and dP/dT. - While able to accommodate volume overload, the right ventricle is poorly adapted for high pressures. Abnormalities in right ventricle size and function













































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
