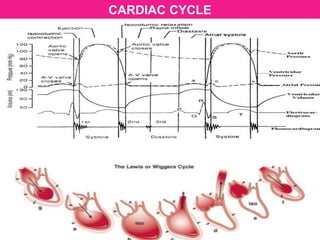
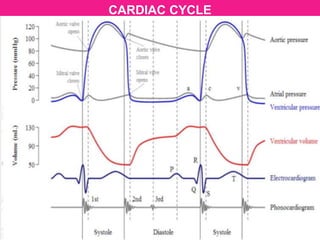
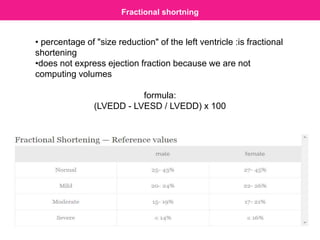
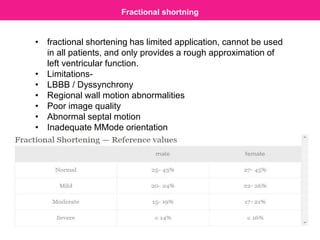
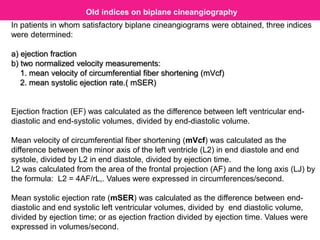
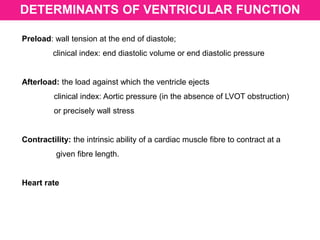
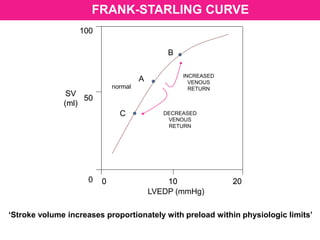
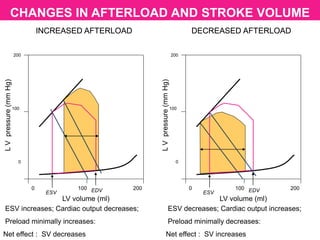
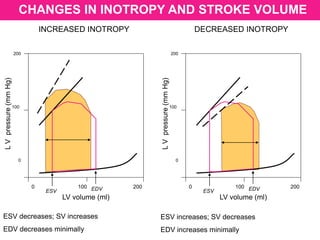
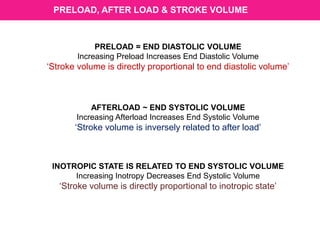
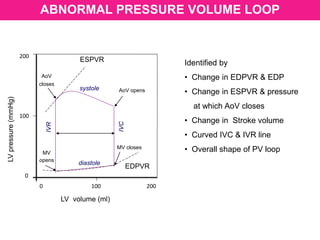
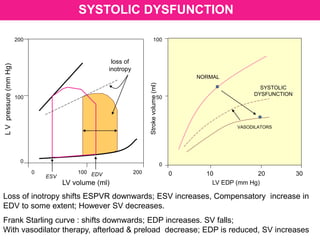
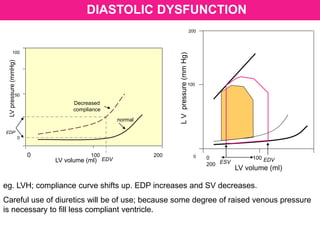
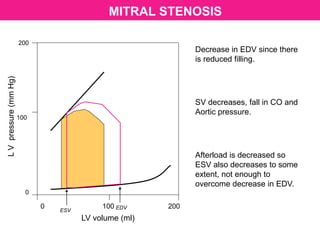
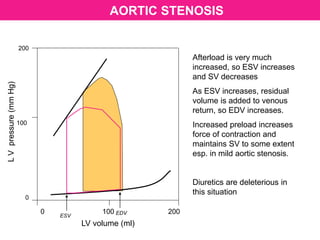
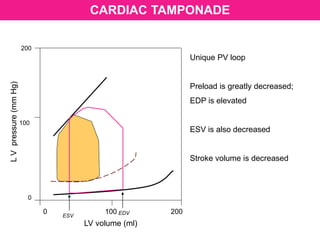
The document discusses ventricular pressure-volume loops and cardiac physiology. It begins by introducing ventricular pressure-volume loops and their use in assessing cardiac function. It then covers the normal cardiac cycle and mechanics, including the isovolumic contraction and relaxation phases. Key concepts like preload, afterload, contractility, compliance, and indices of cardiac function such as ejection fraction, fractional shortening, and Tei index are defined and their clinical significance explained. Older indices assessed by biplane cineangiography are also mentioned.








































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)



![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)










