Downloaded 116 times
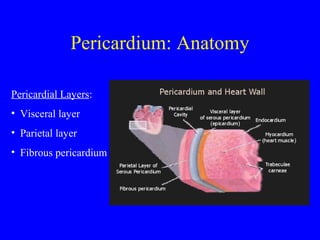
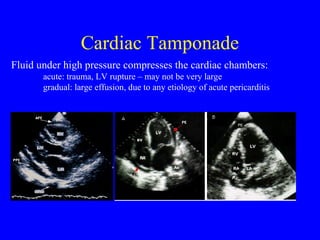
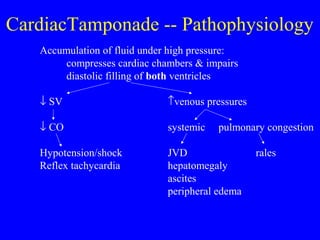
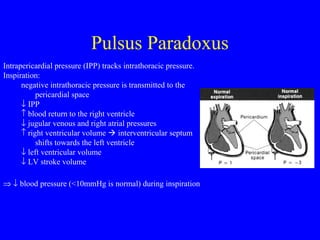
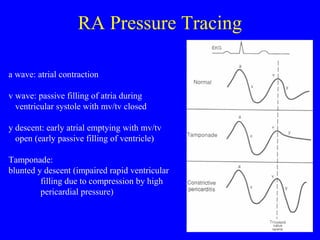
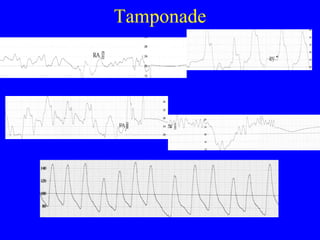
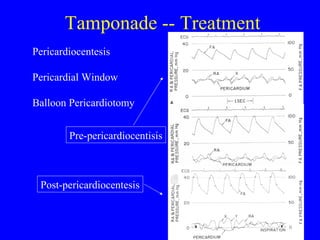

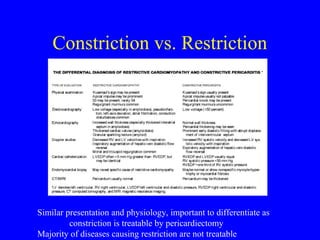

The document discusses the anatomy, functions, pathophysiology, etiologies, clinical features, diagnosis and treatment of pericardial diseases including pericarditis, pericardial effusion, cardiac tamponade, and constrictive pericarditis. Key points include: the pericardium has visceral and parietal layers separated by pericardial fluid; pericarditis can be caused by infection, autoimmune disorders, neoplasms or trauma; tamponade occurs when fluid rapidly accumulates under pressure, compressing the heart; constrictive pericarditis involves fibrosis and scarring that restricts diastolic filling.























































































