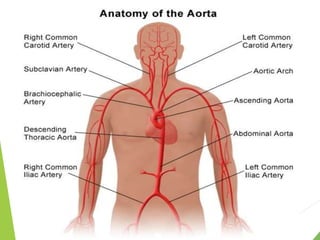
The aorta is the main artery that carries oxygenated blood from the heart to the rest of the body. It originates from the left ventricle and splits into the common iliac arteries in the abdomen. The aorta is divided into four sections - the ascending aorta, aortic arch, descending aorta, and abdominal aorta. It supplies blood to the entire body except the lungs. The aorta is composed of three layers - the tunica intima, tunica media, and tunica adventitia. Common conditions of the aorta include aneurysms, which involve abnormal dilations, and coarctation, which is a narrowing of the aorta.