Downloaded 474 times

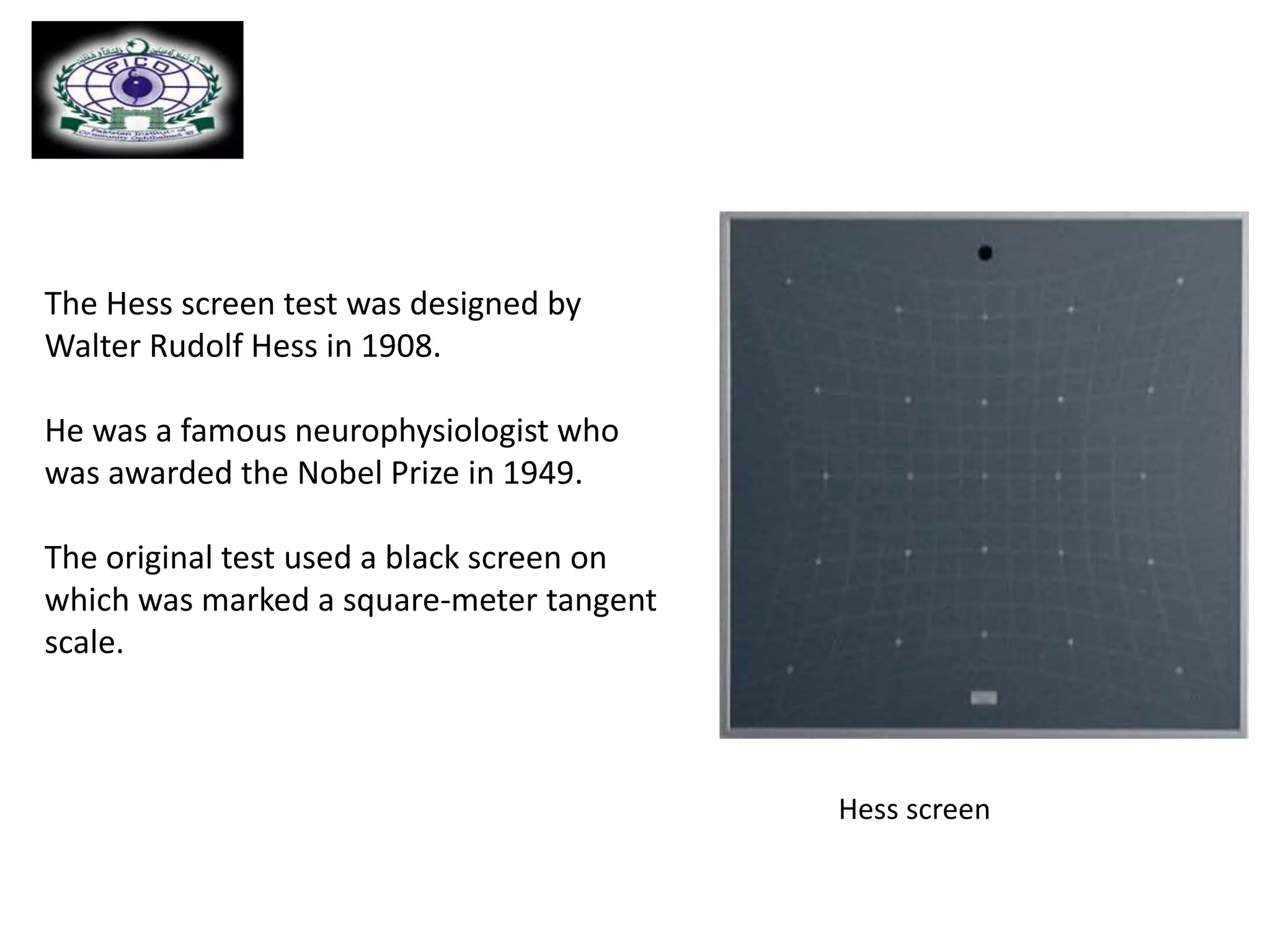




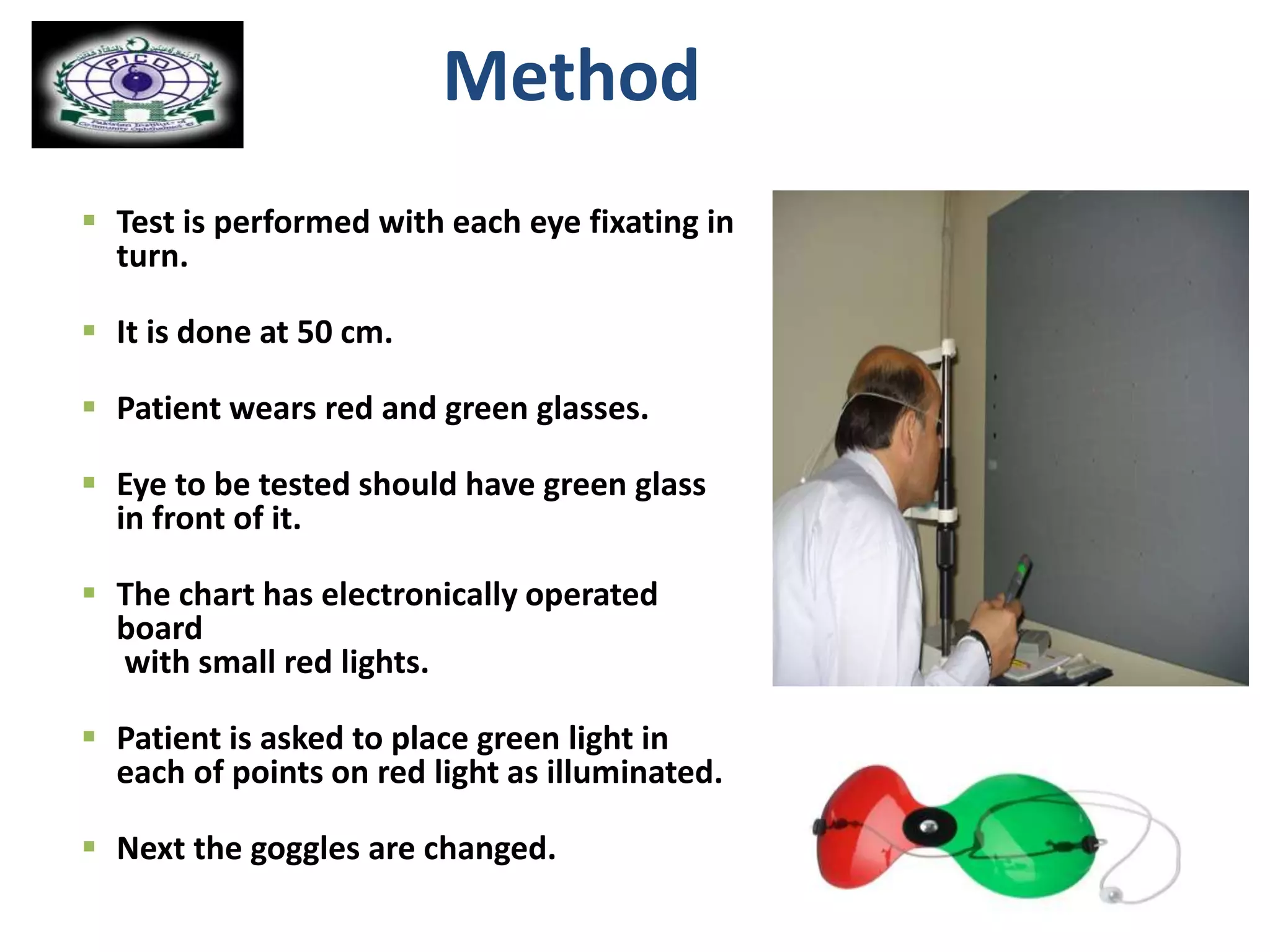












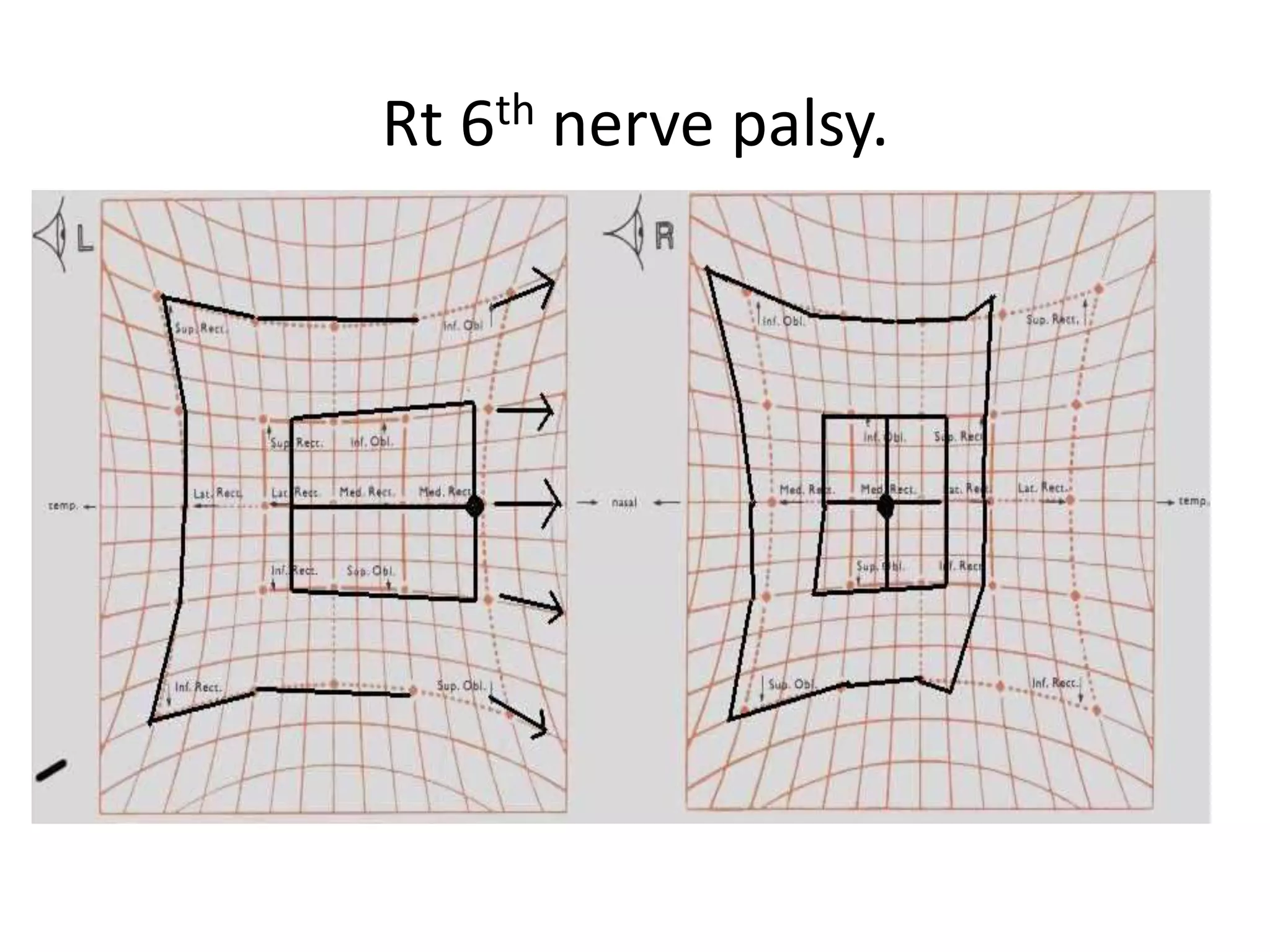

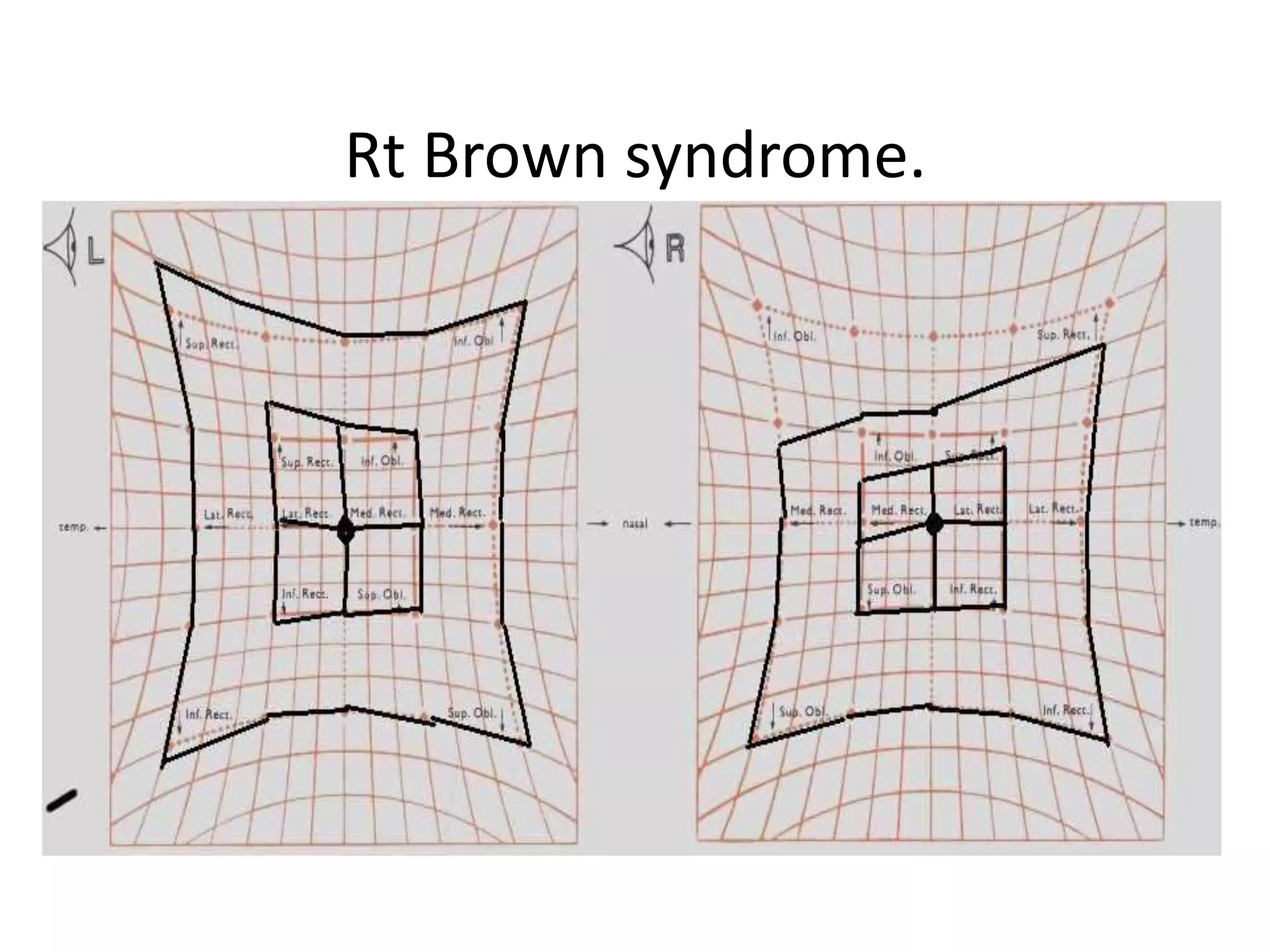


The Hess screen test is used to evaluate eye muscle function and diagnose abnormalities. It involves the patient fixating on lights illuminated on a screen while wearing colored lenses over each eye. Patterns in how the lights are seen can reveal underaction or overaction of extraocular muscles, and determine if a deviation is comitant or incomitant. The test allows diagnosis of conditions like neurogenic or mechanical palsies, and helps evaluate their effects over time and before/after surgery. Interpretation involves analyzing features like the size and direction of any deviation, whether fields are similar between eyes, and if patterns indicate particular affected muscles or nerves.






























































































