Downloaded 16 times














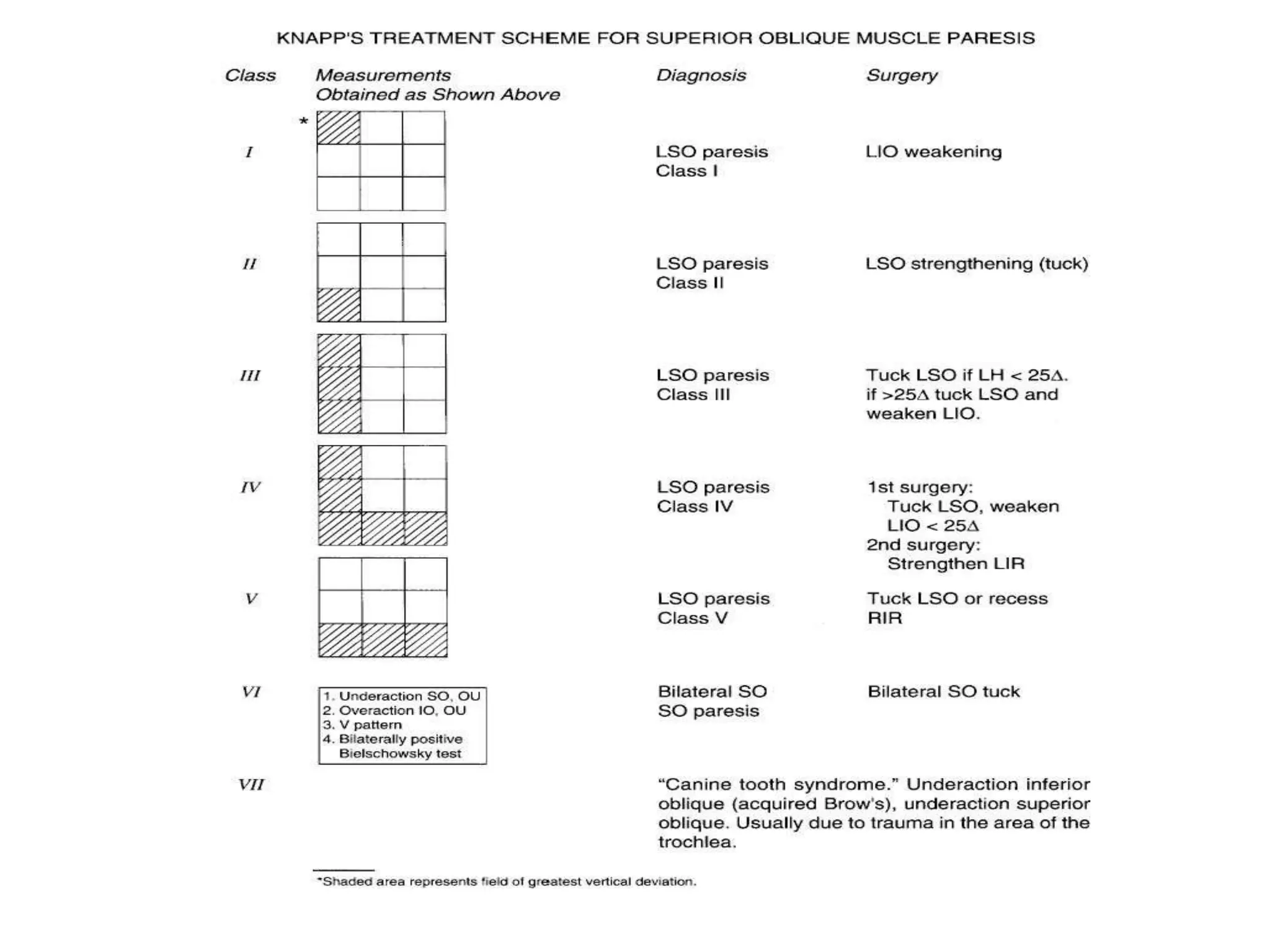
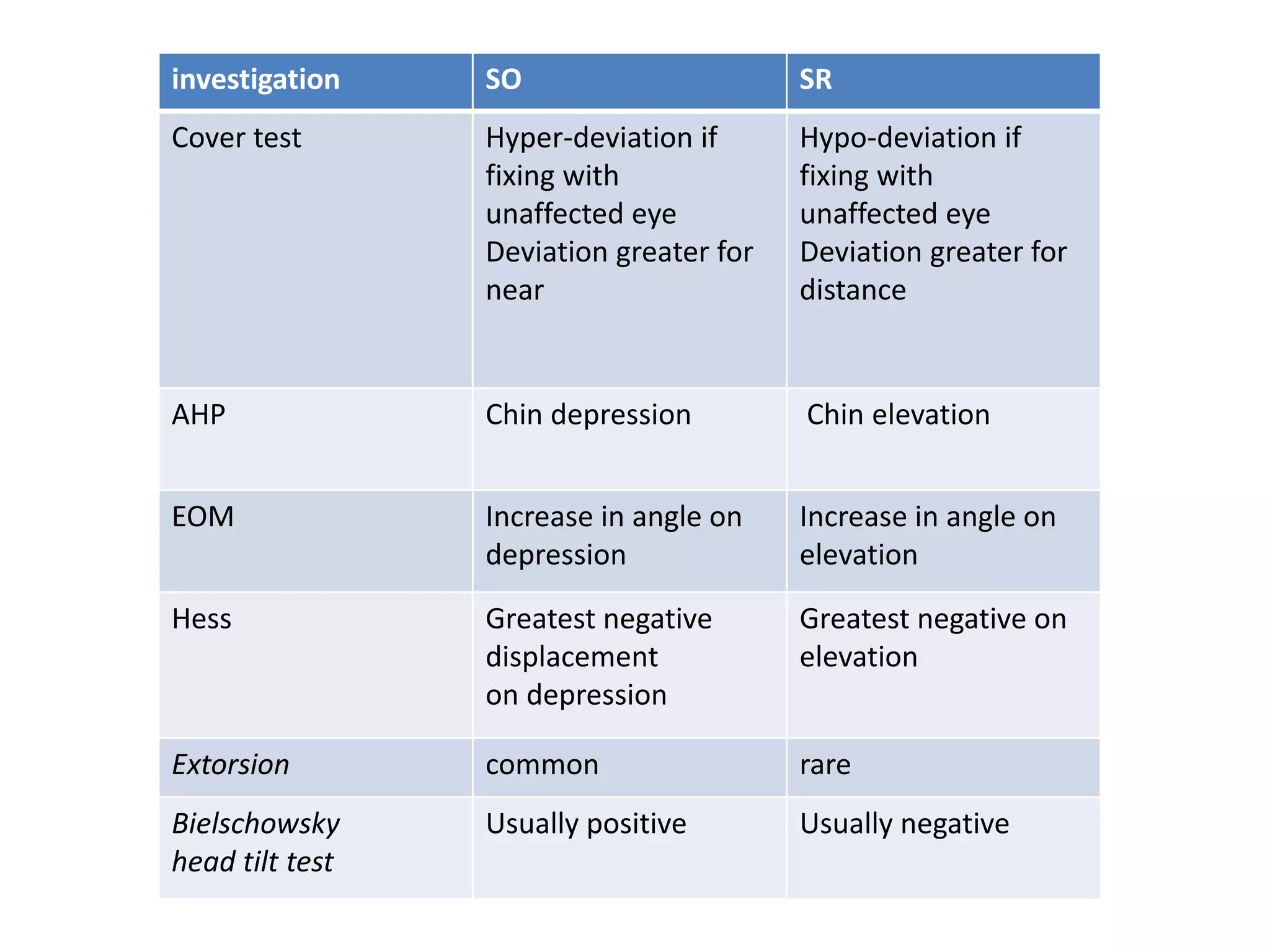
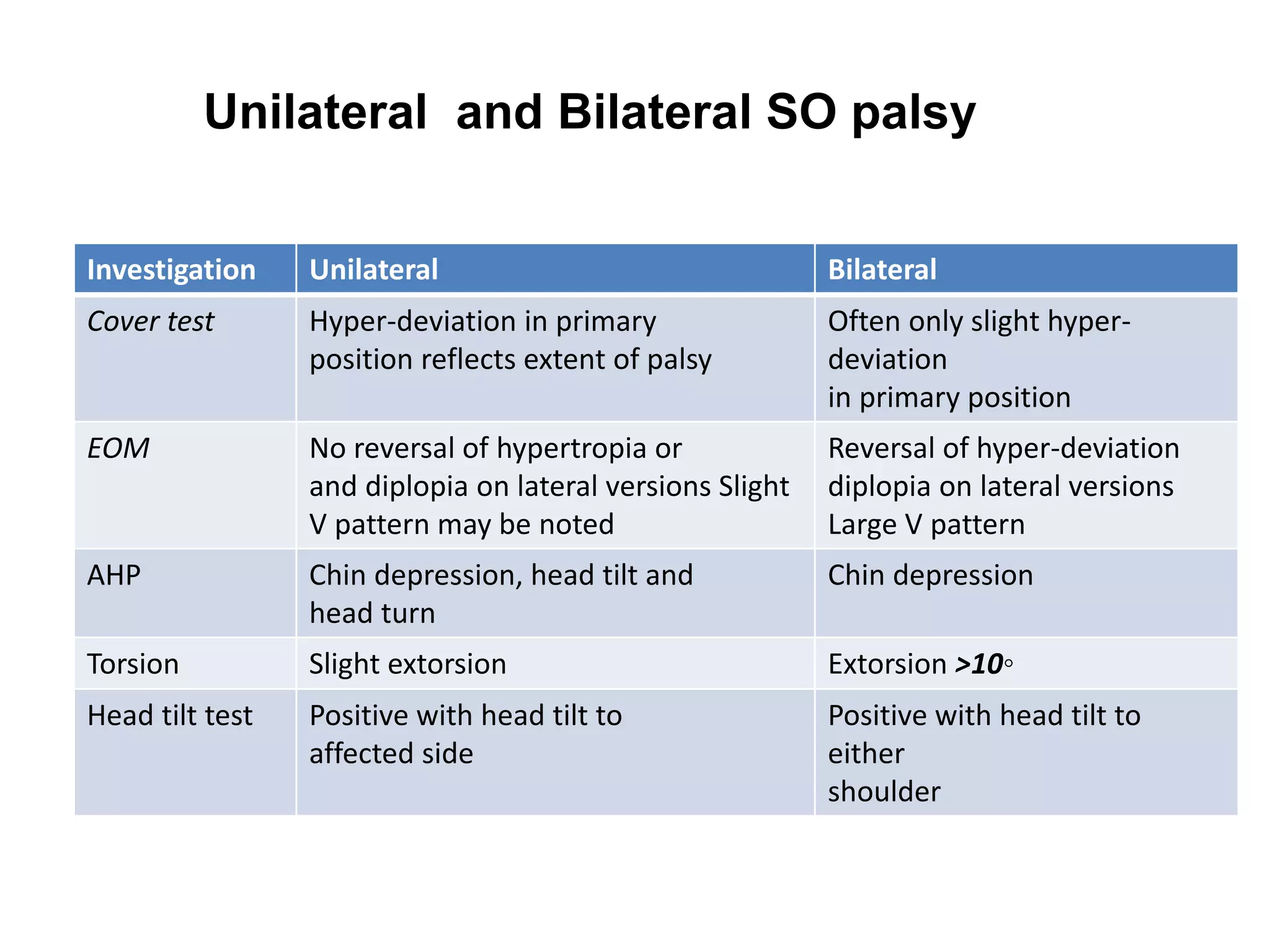


The document discusses Fourth Nerve Palsy (SOP), which causes weakness of the superior oblique muscle. It describes the anatomy of the fourth cranial nerve and the effects of SOP, including ipsilateral hypertropia that increases in opposite gaze. Common causes are trauma, vascular issues like hypertension, and diabetes. Clinical findings are outlined, along with classification systems. Management involves investigating for underlying causes, using prisms for small deviations, and surgery like weakening overacting muscles for large deviations. Surgical techniques are provided to address specific muscle weaknesses or torsion.













































































