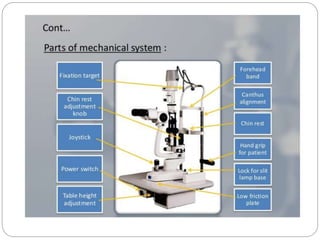
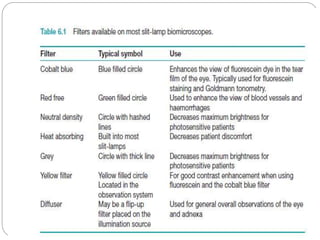
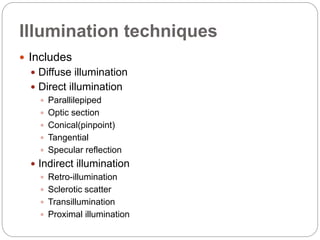
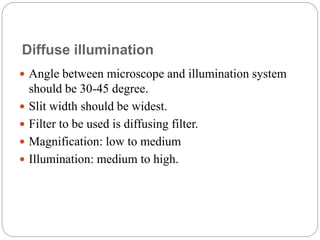
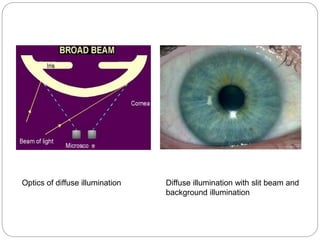
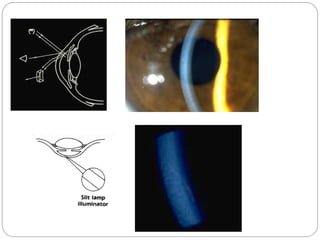
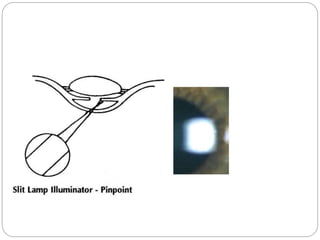
The document discusses slit lamp examinations, which use a high-intensity light source focused as a slit and viewed through a microscope to examine the anterior segment of the eye. It describes the basic components and principles of the slit lamp biomicroscope, various illumination techniques used to examine different ocular structures, and historical developments of the slit lamp.