Downloaded 15 times
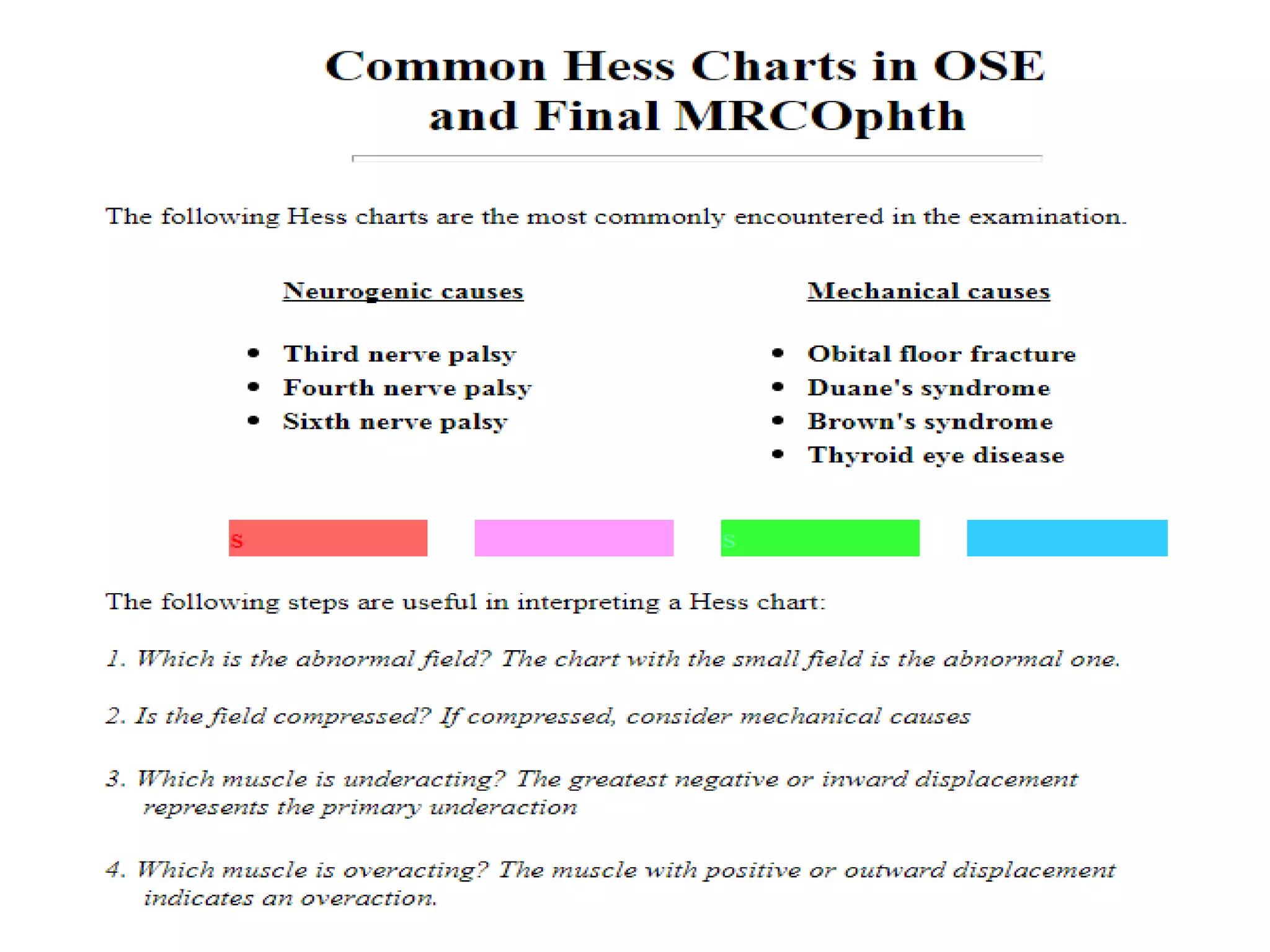
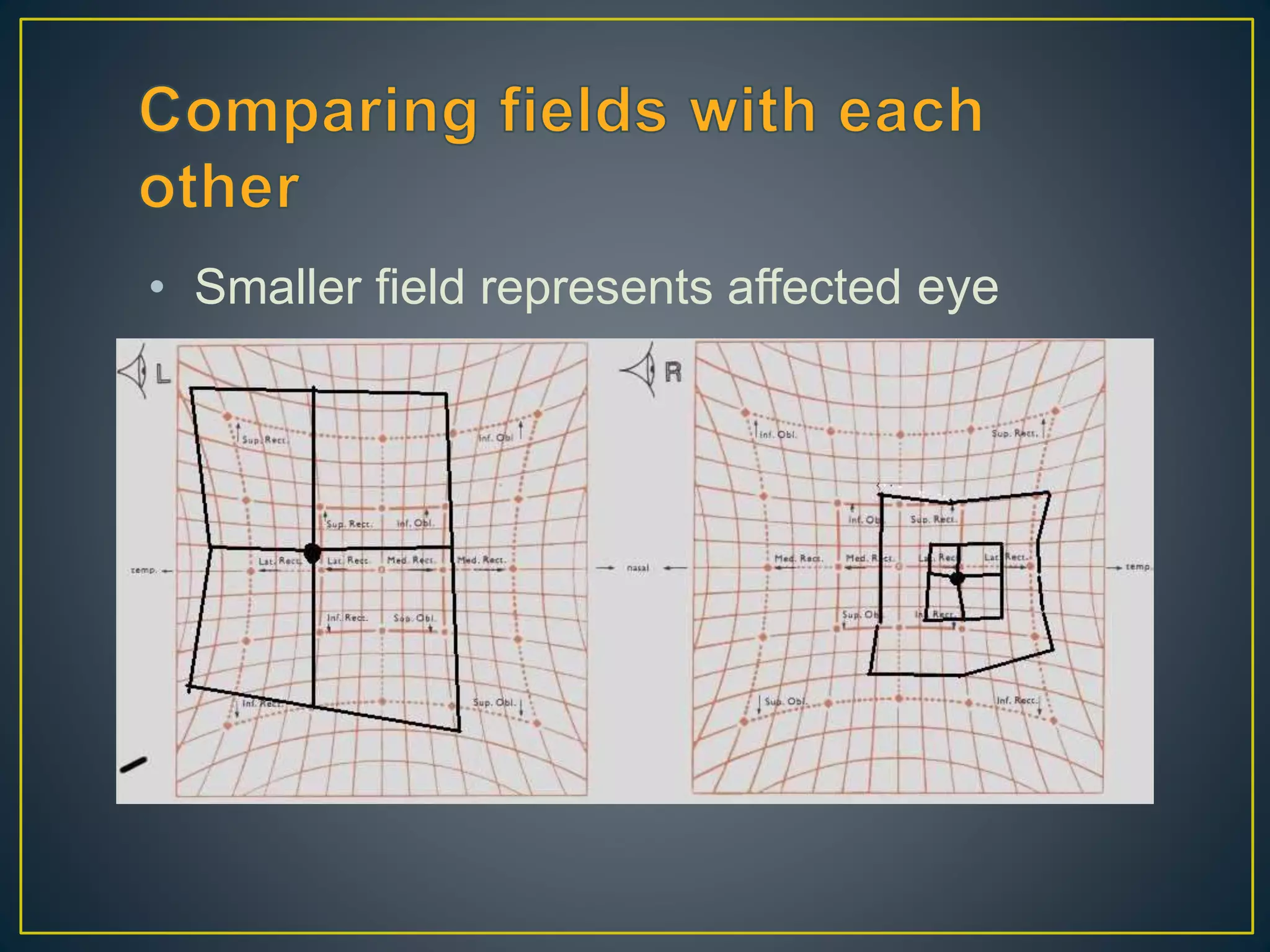
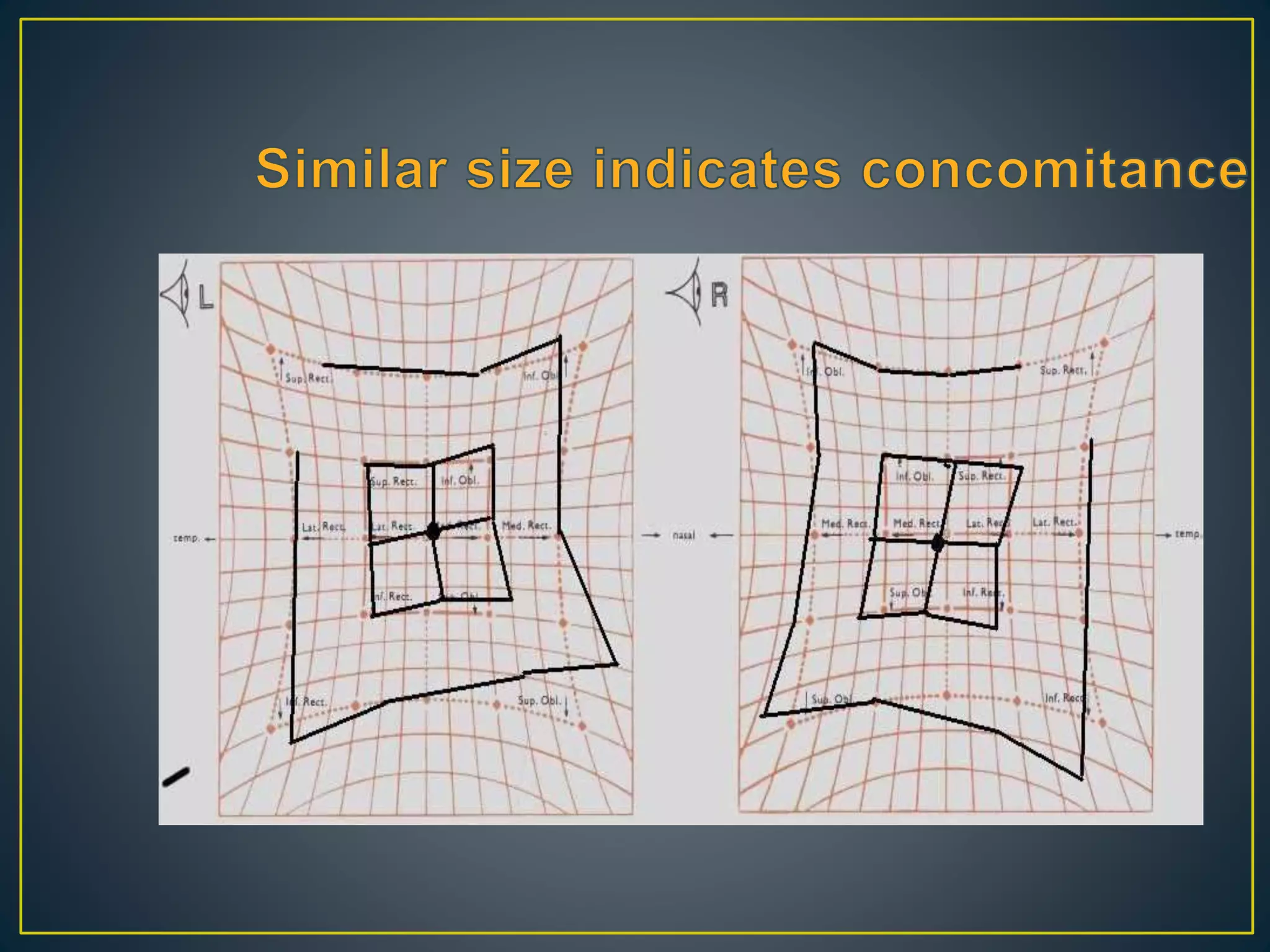
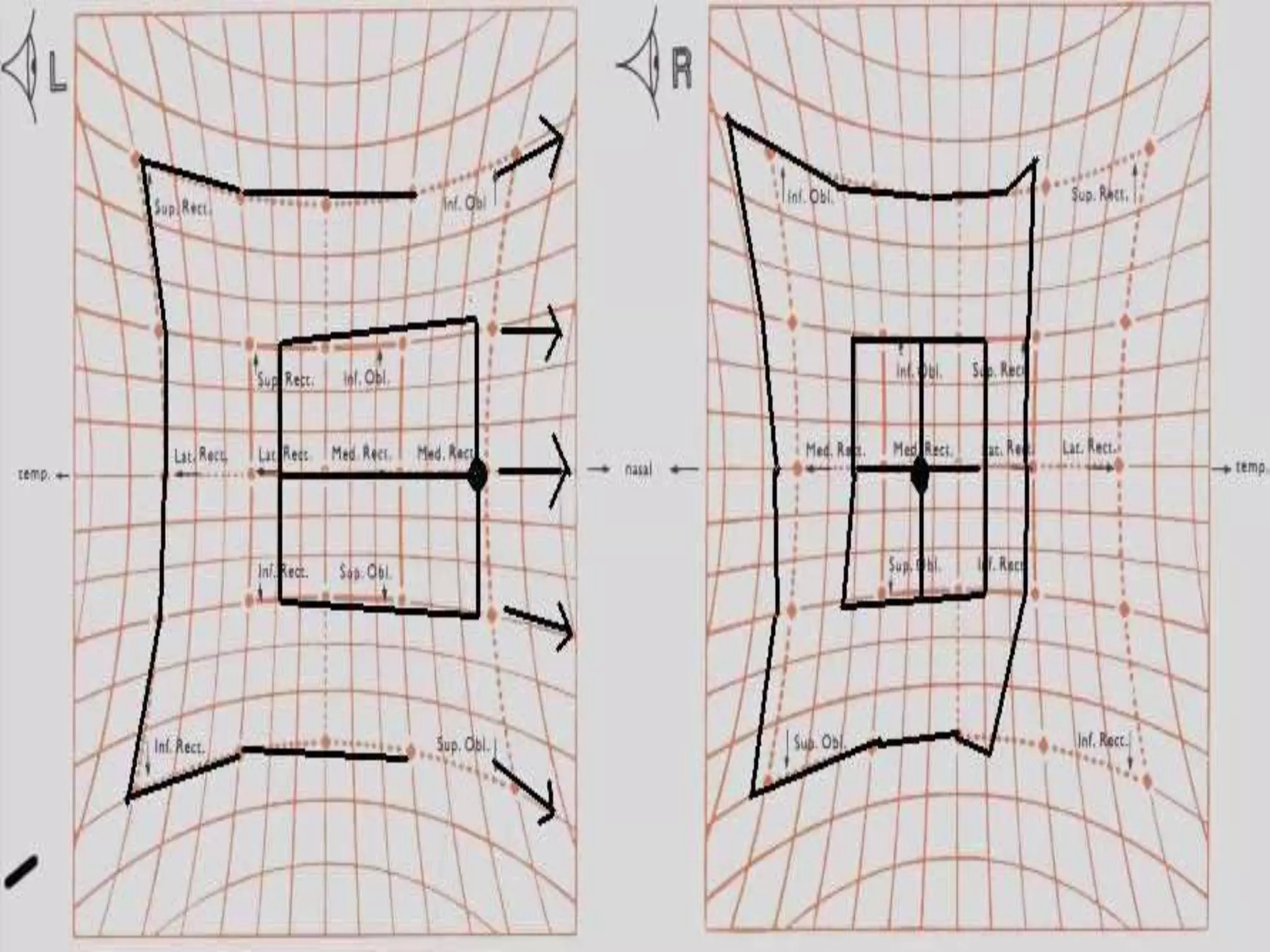
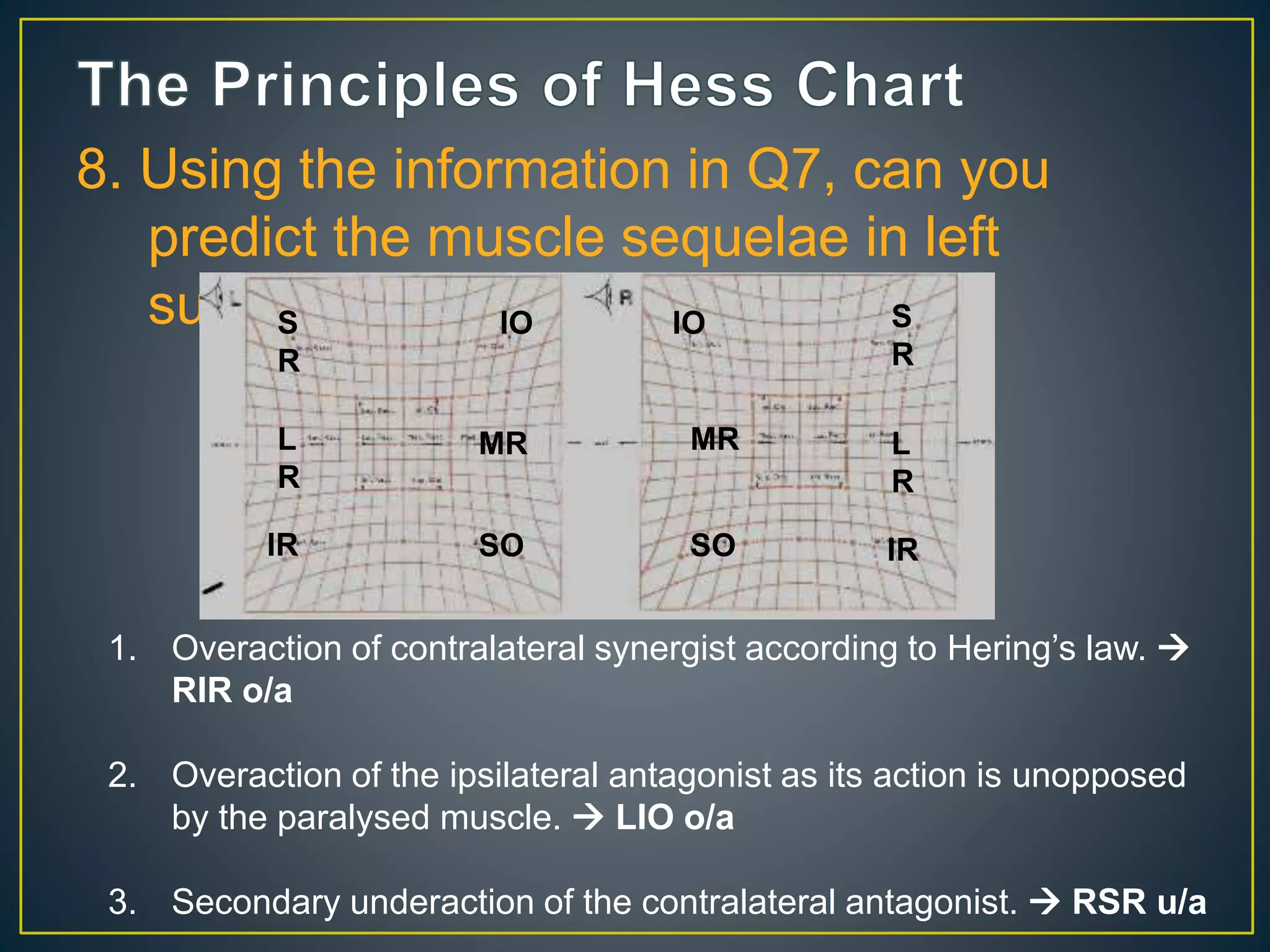
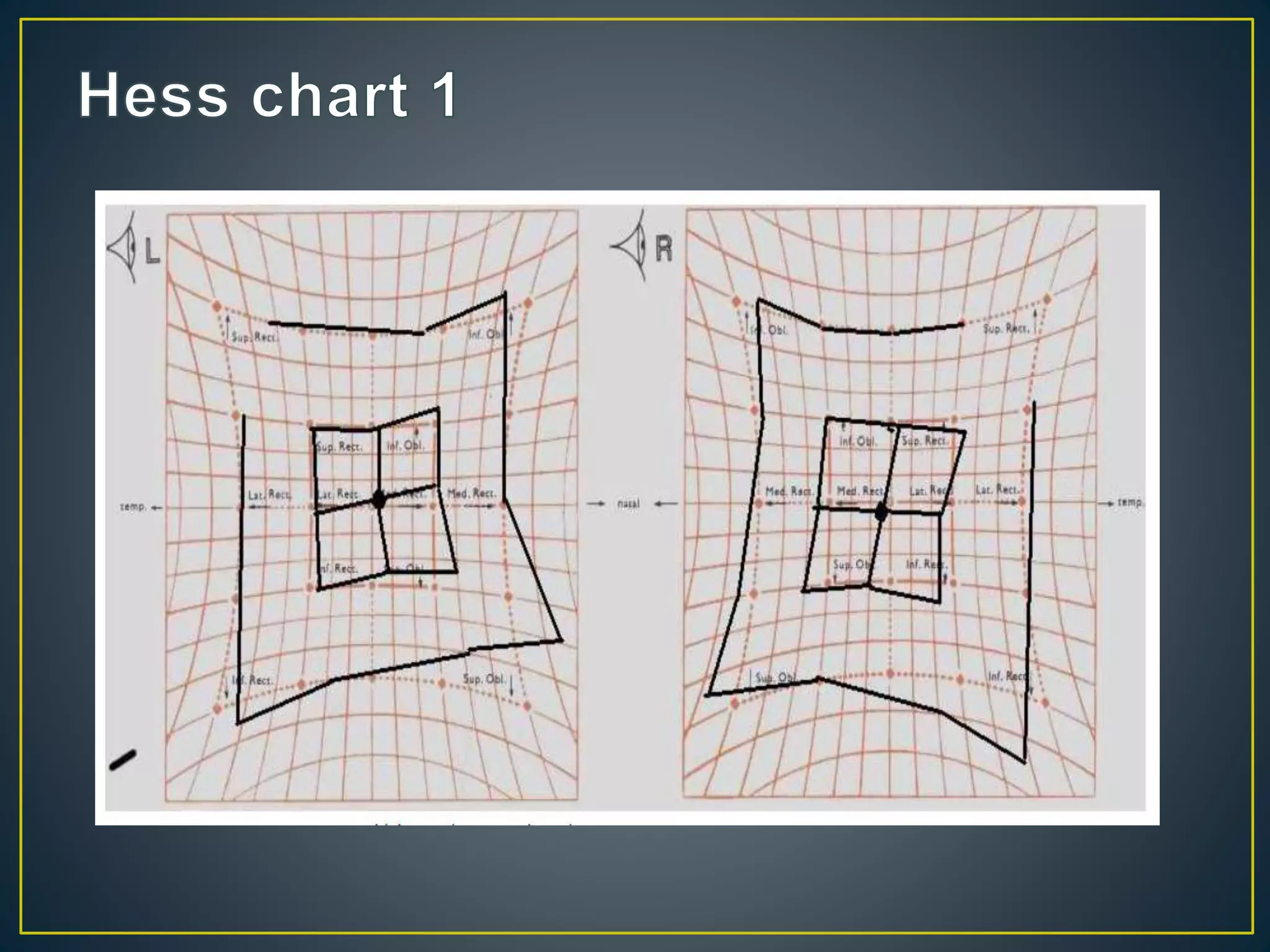
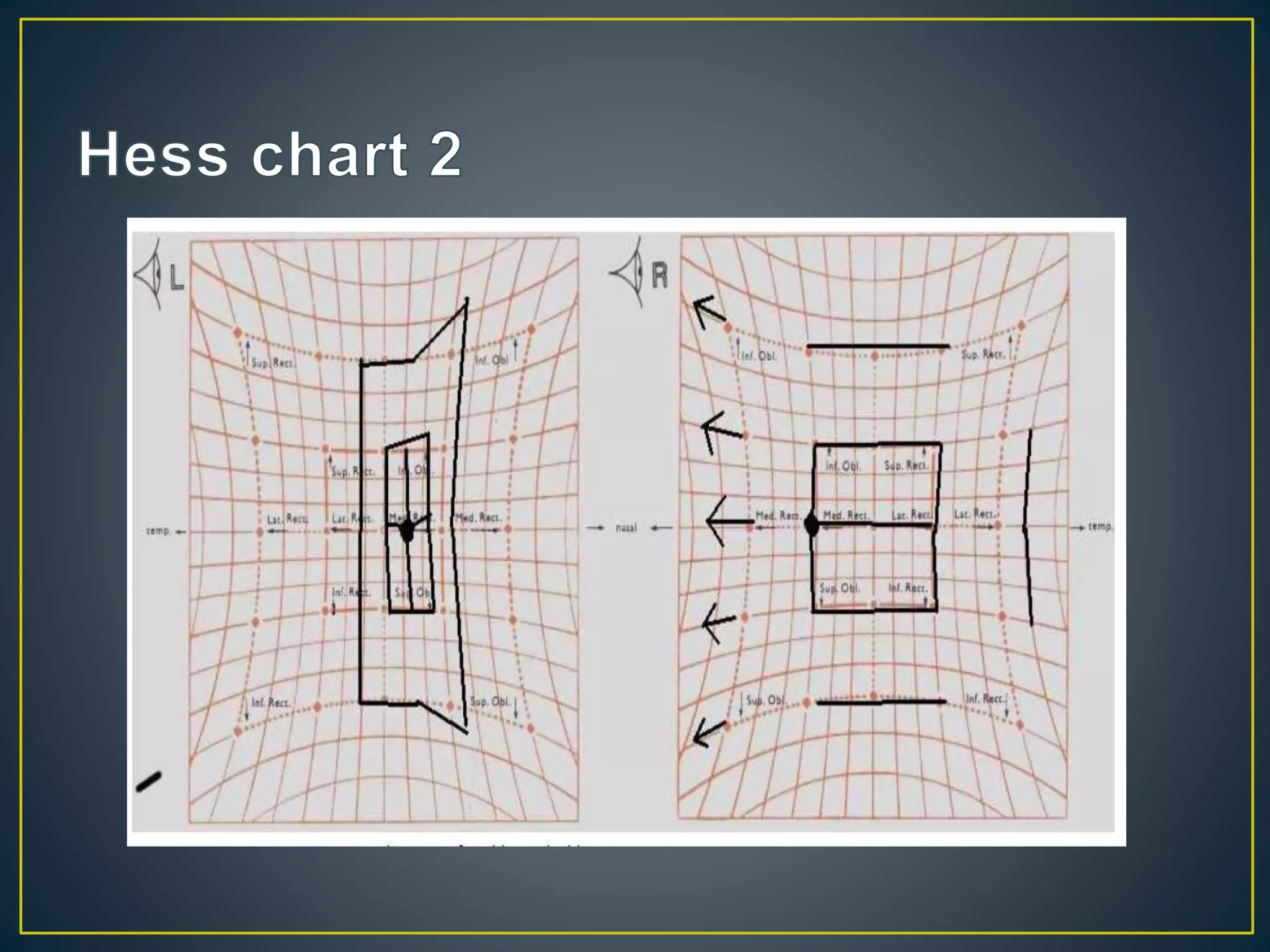
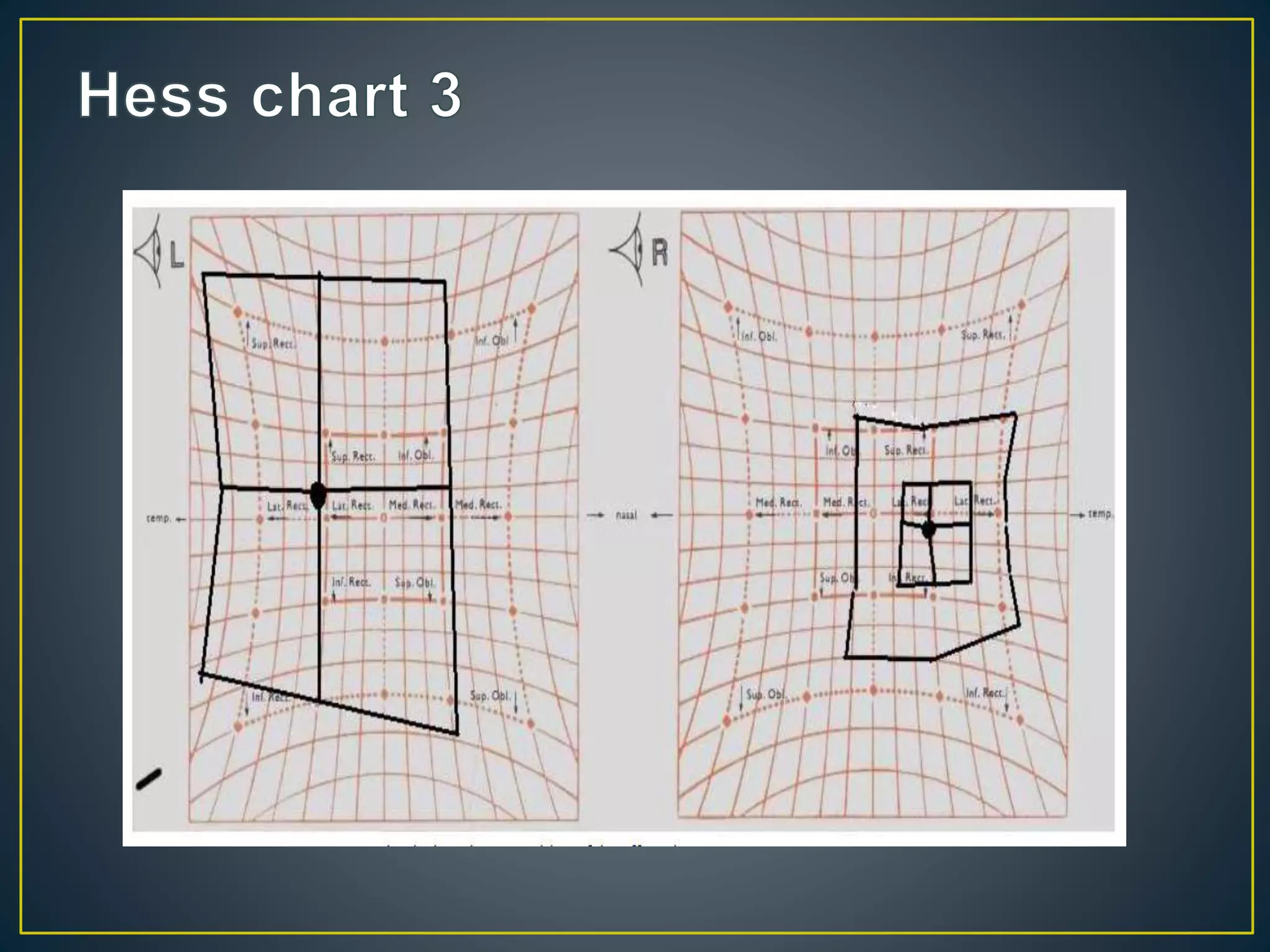
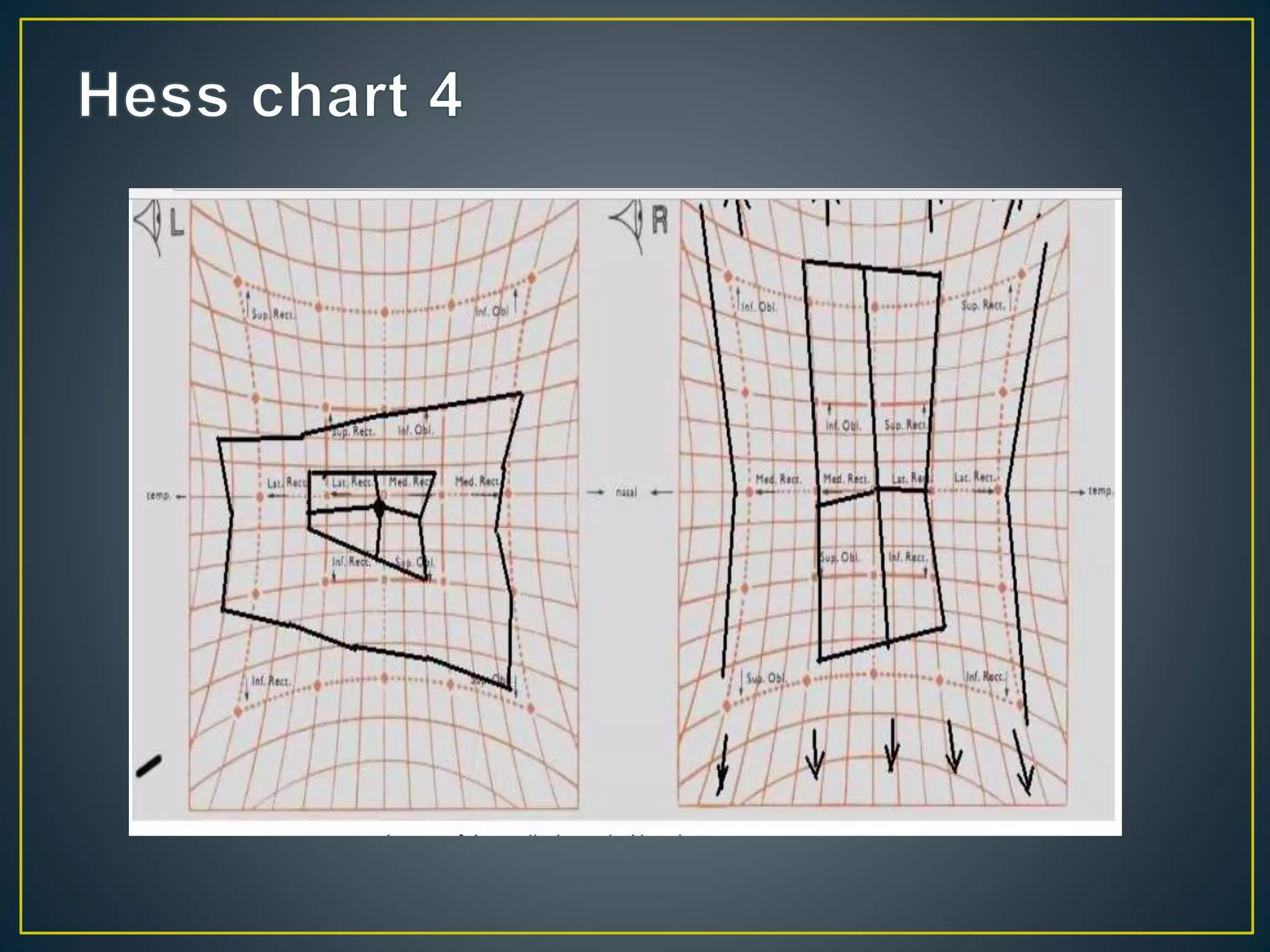
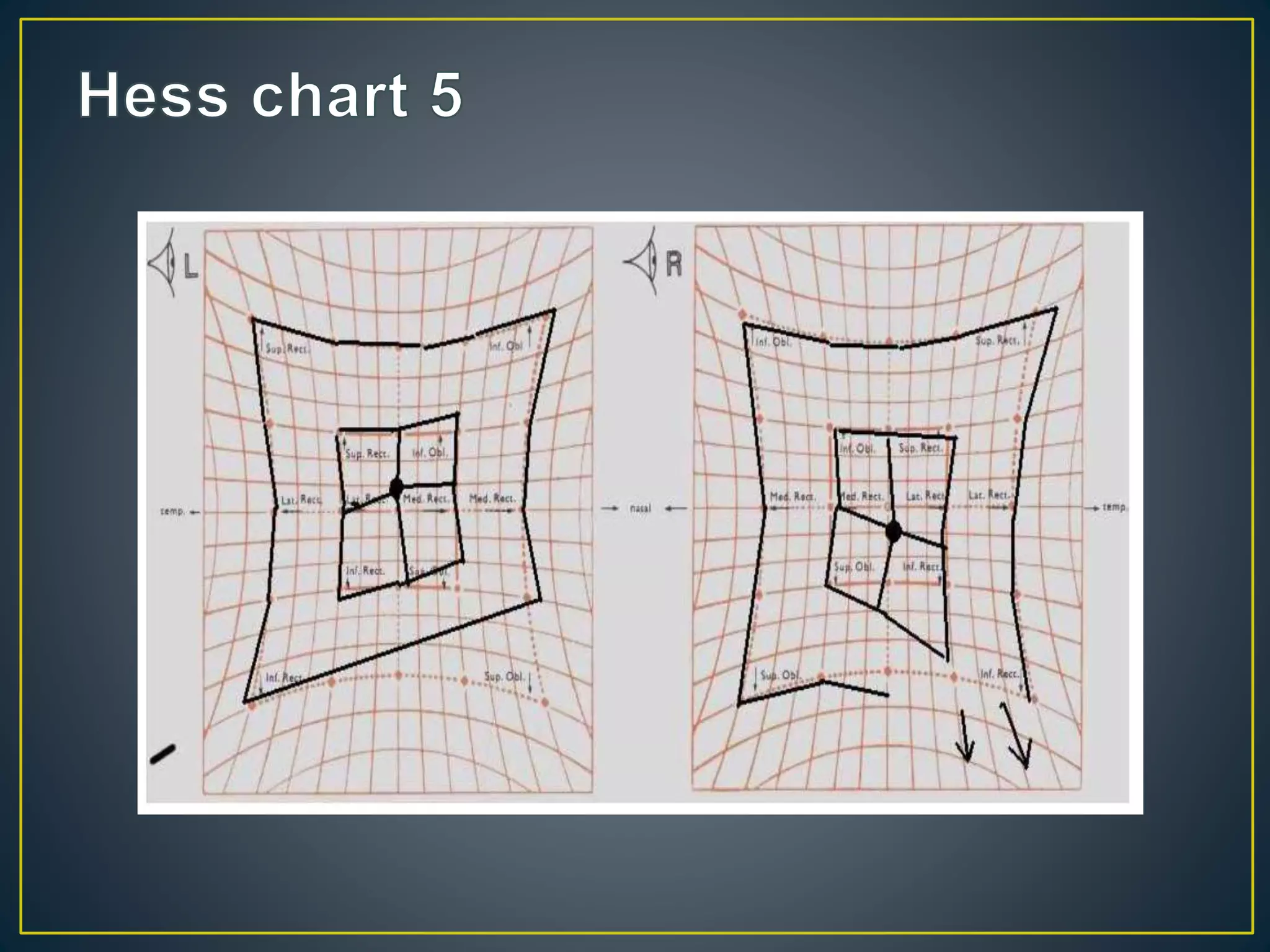
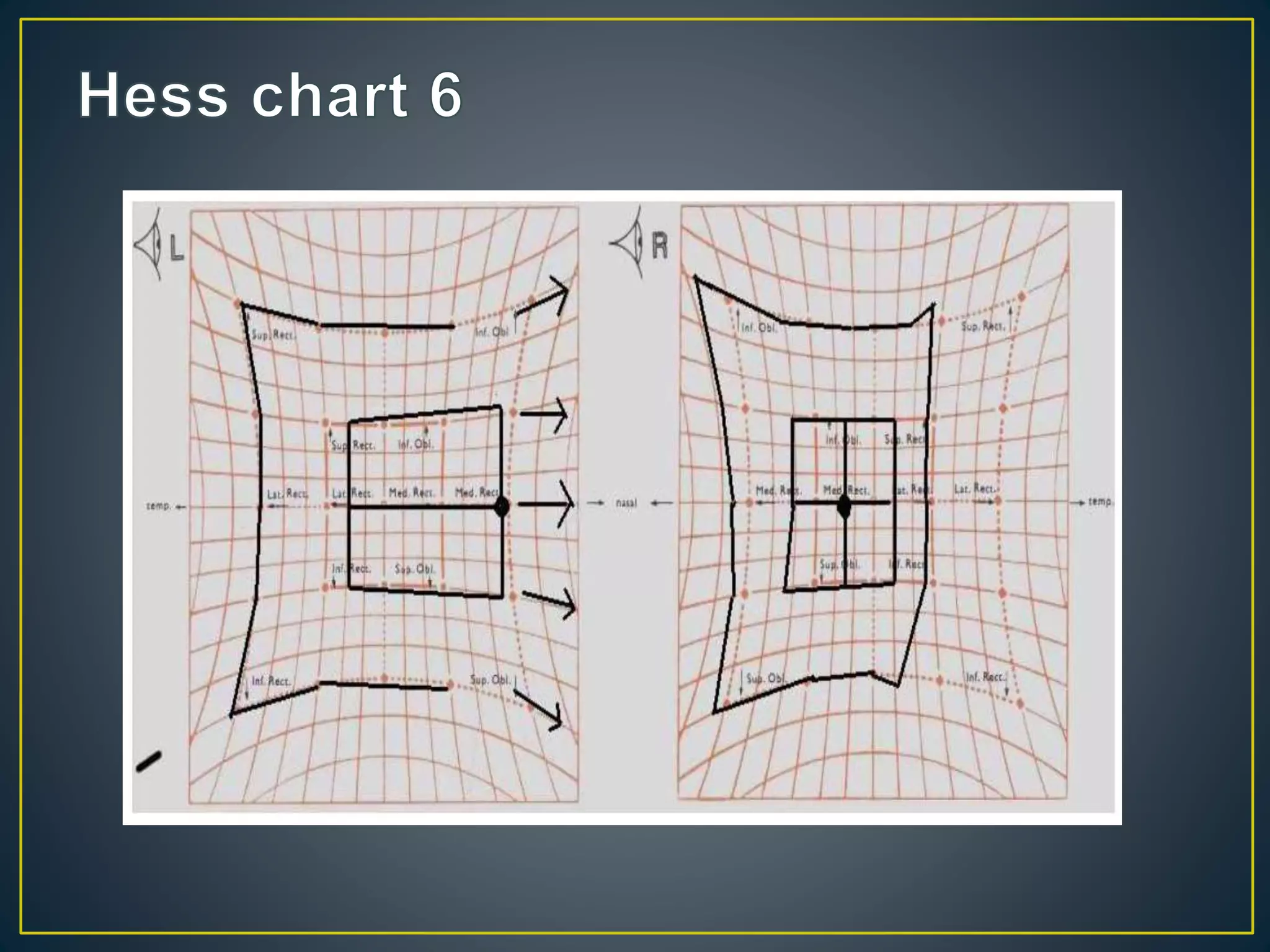

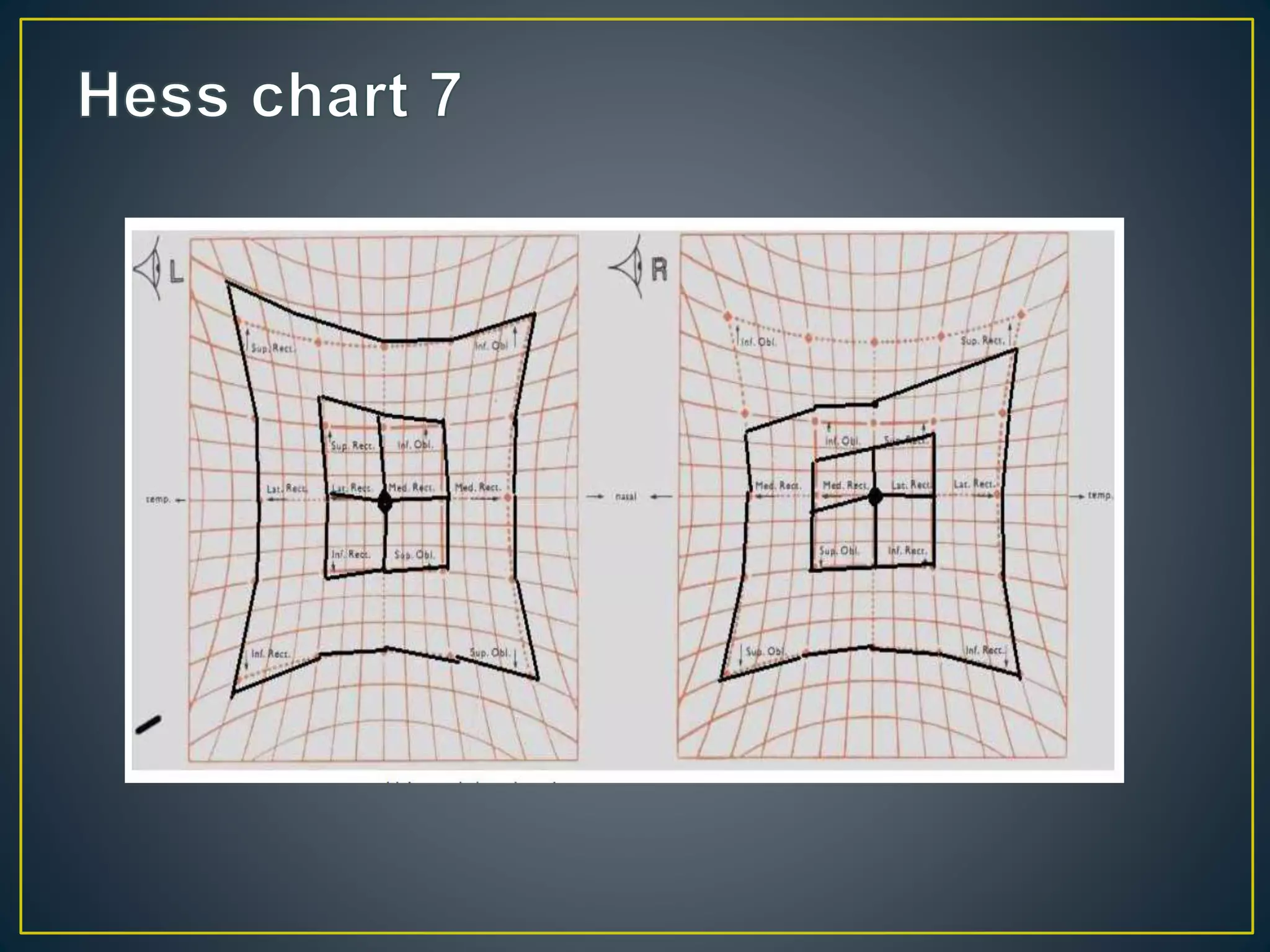

The Hess chart provides information about eye movements and deviations in different gazes. Key features include the size and shape of the fields, positions of the central dots indicating deviations, and displacements showing underactions and overactions. Together these can indicate the affected eye and muscle(s), type of strabismus, whether it is recent or longstanding, and help make a diagnosis such as thyroid eye disease or cranial nerve palsy. Hess charts are useful for monitoring changes over time both clinically and following strabismus surgery.























































































