Downloaded 469 times
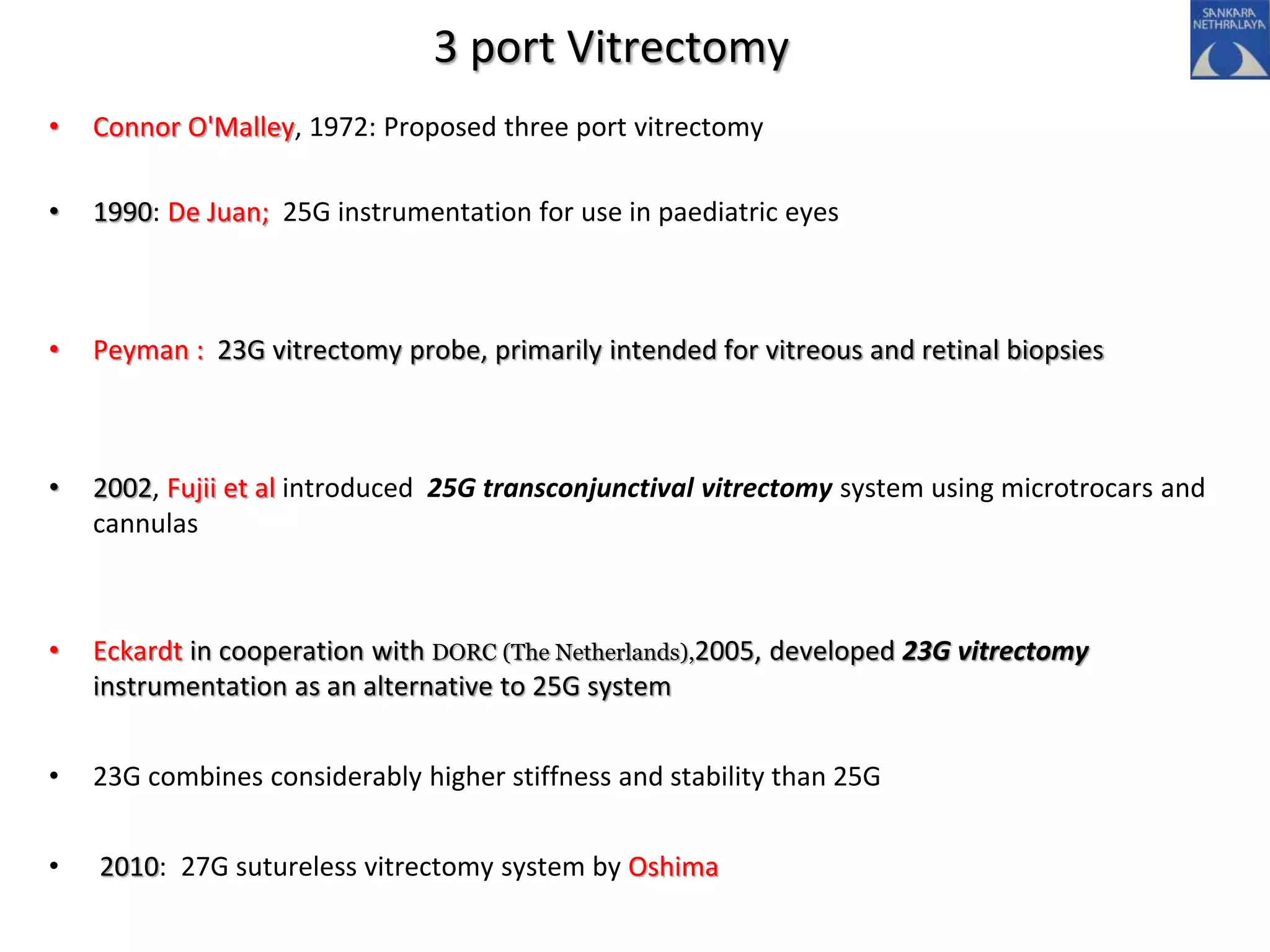
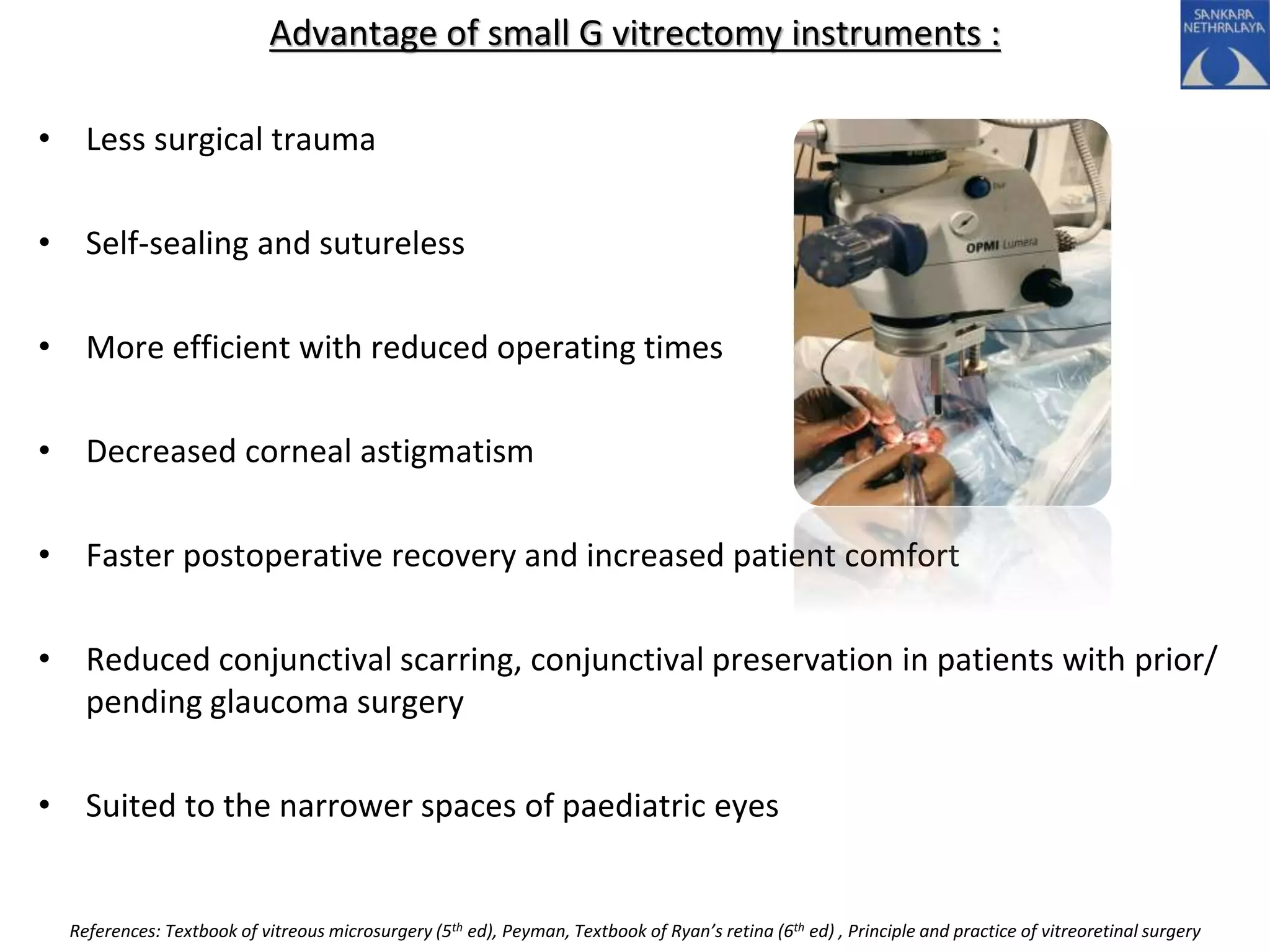
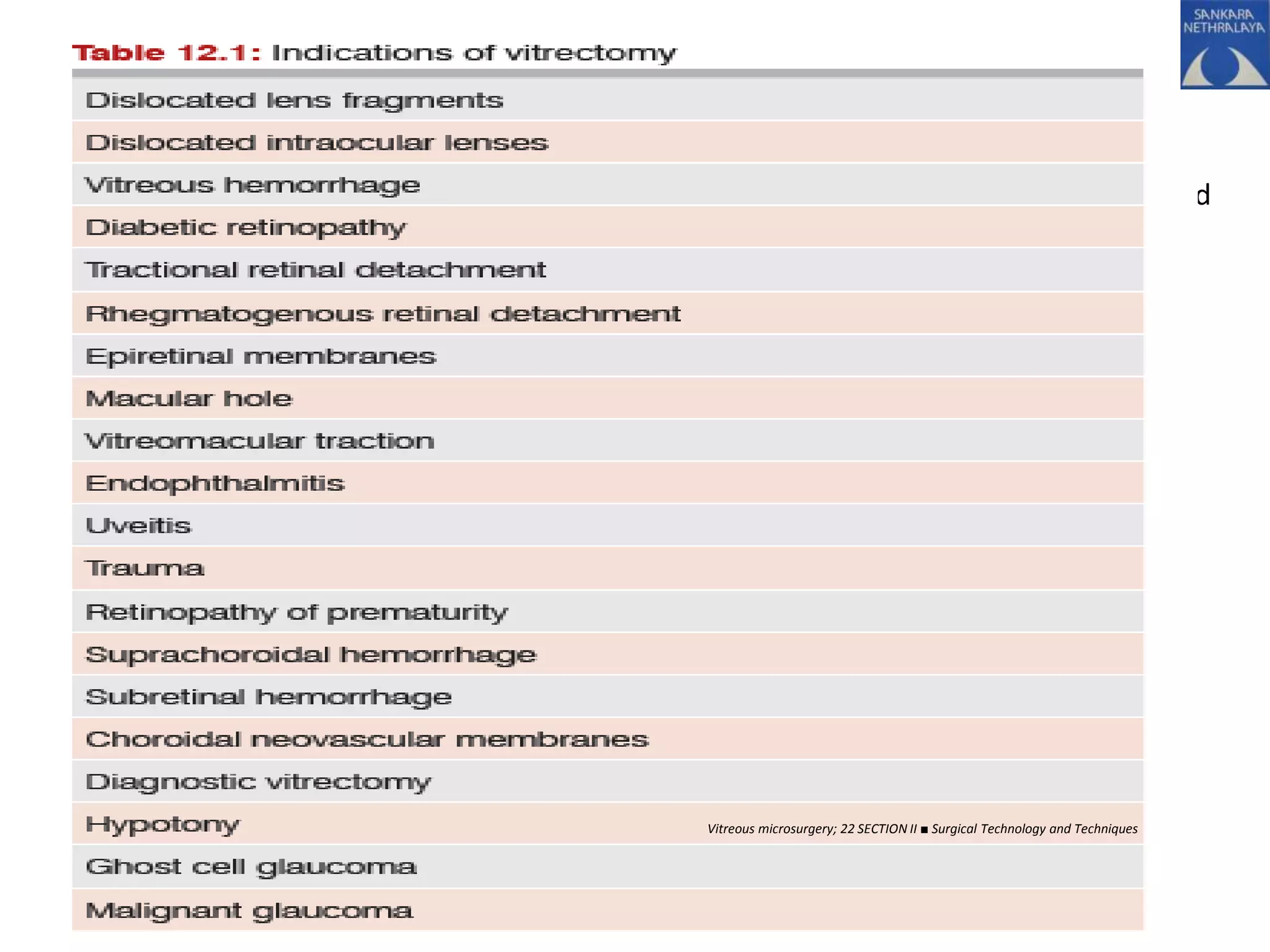
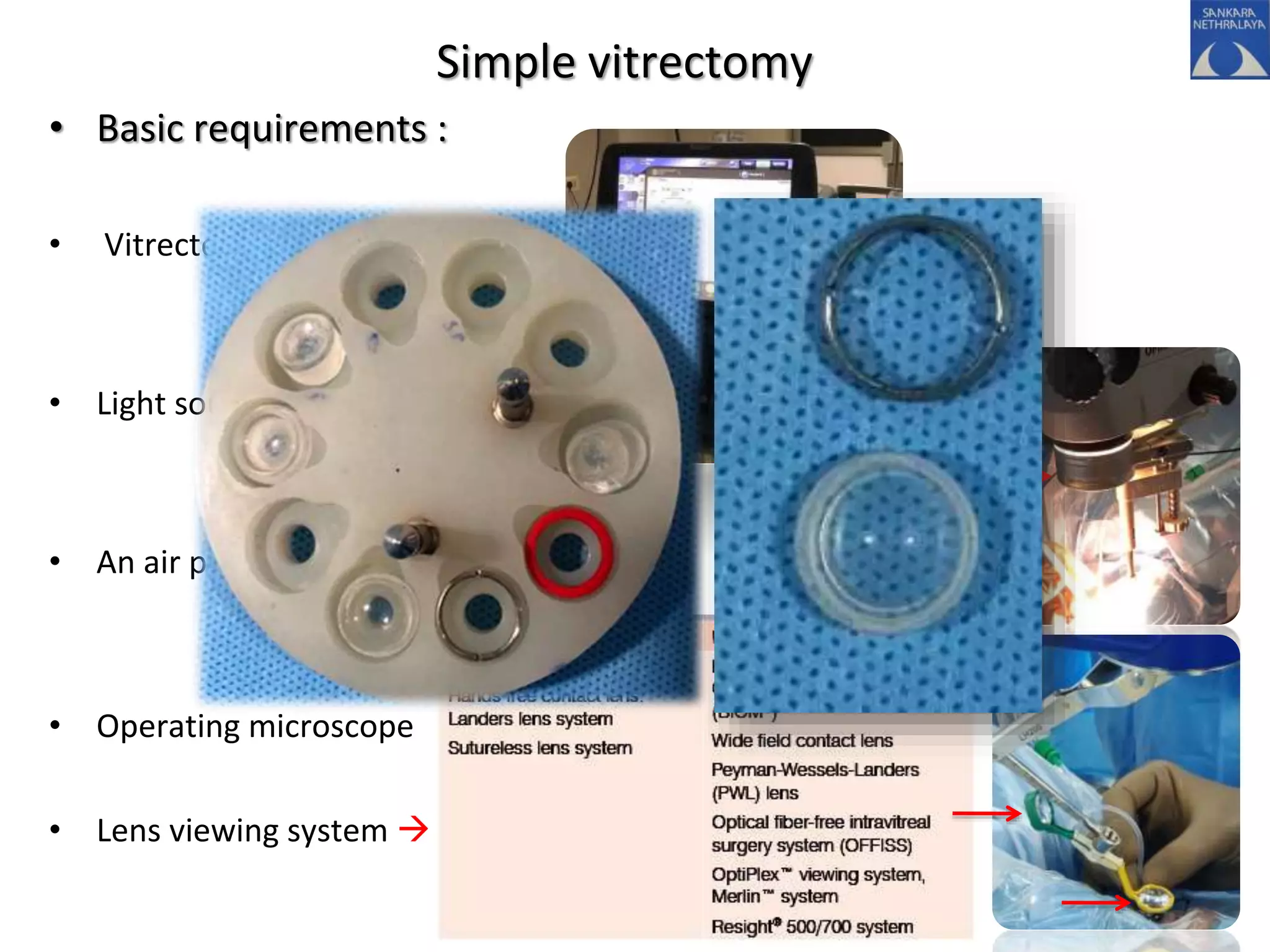
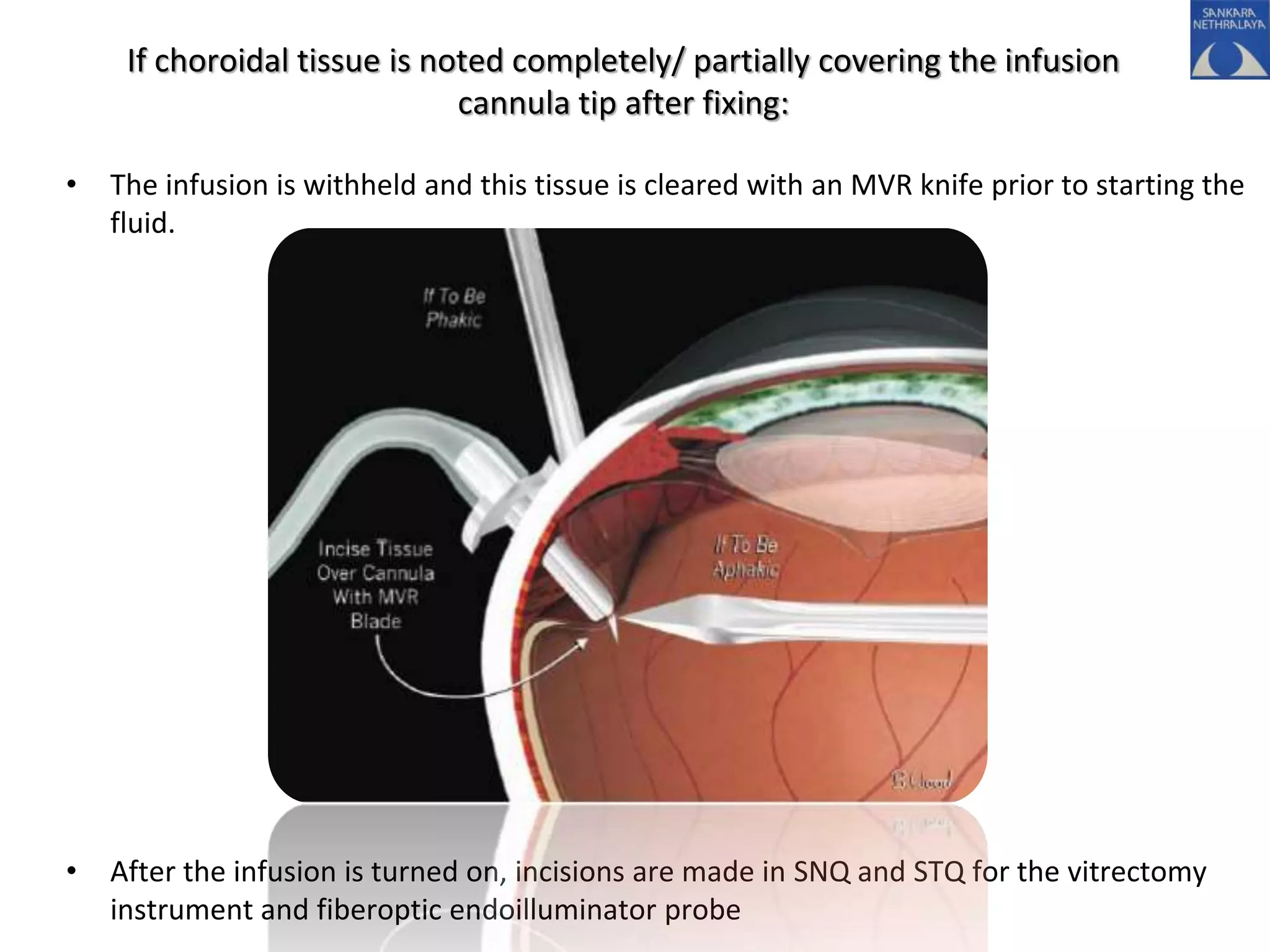



This document provides an overview of vitrectomy, including a brief history, the key steps in a simple vitrectomy procedure, and descriptions of the equipment used. It discusses trocars and cannulas, sclerotomies, illumination sources, viewing systems, vitreous cutters, and vitreous removal. Advantages of smaller gauge vitrectomy instruments are also summarized.






































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
















