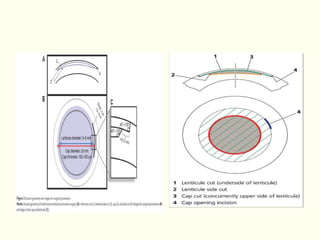
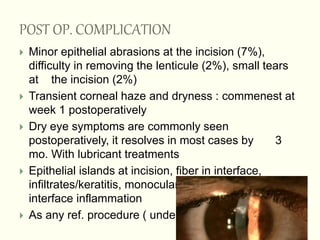
ReLEx SMILE is a new flapless and bladeless refractive eye surgery procedure that treats myopia, hyperopia, astigmatism, and presbyopia using a femtosecond laser to extract a corneal lenticule through a small incision. The procedure has demonstrated efficacy with high predictability and safety, with a significant percentage of eyes maintaining or improving their vision postoperatively. Complications are generally minor, though transient symptoms like dry eyes and corneal haze may occur, resolving in most cases within three months.