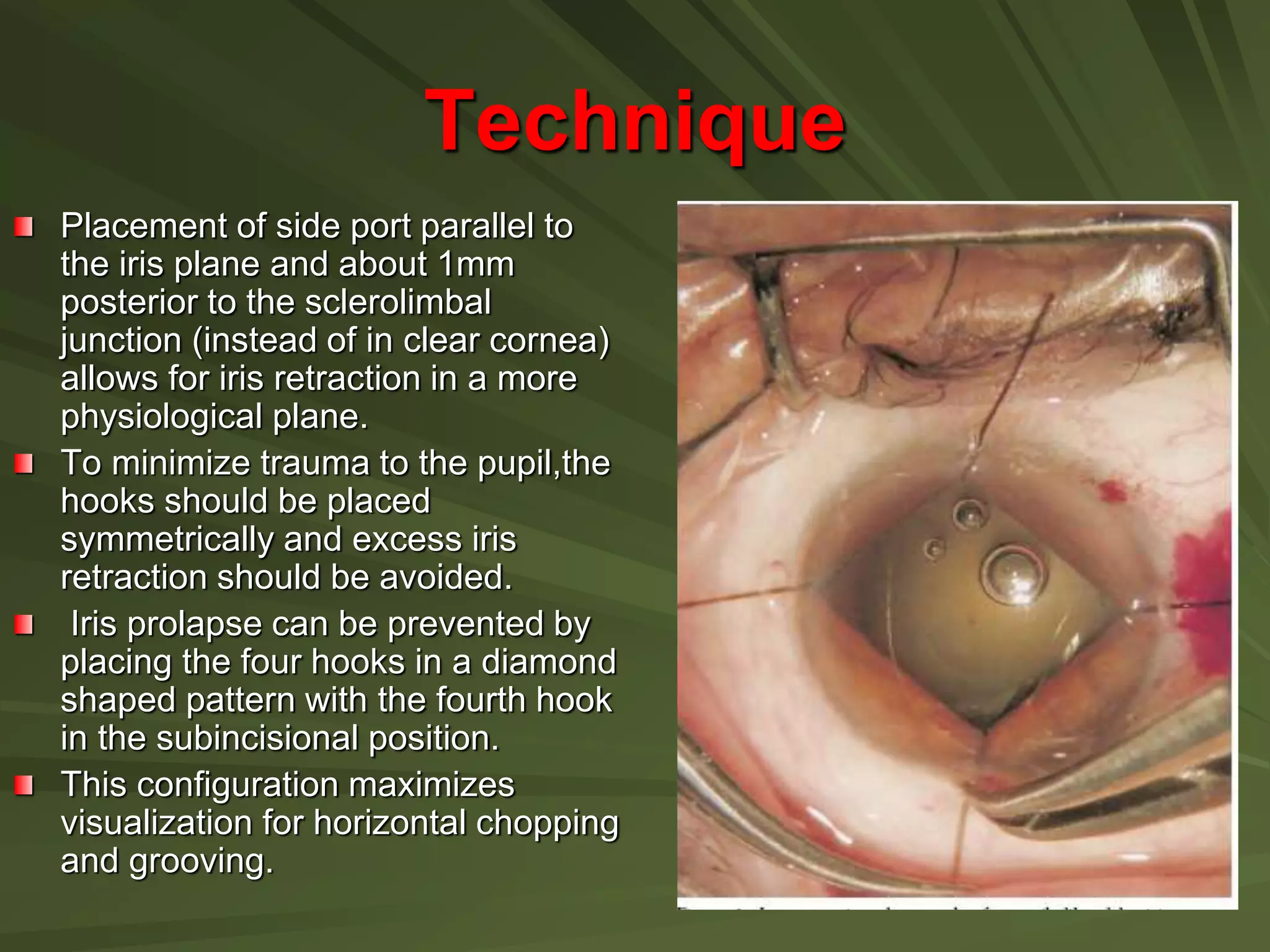
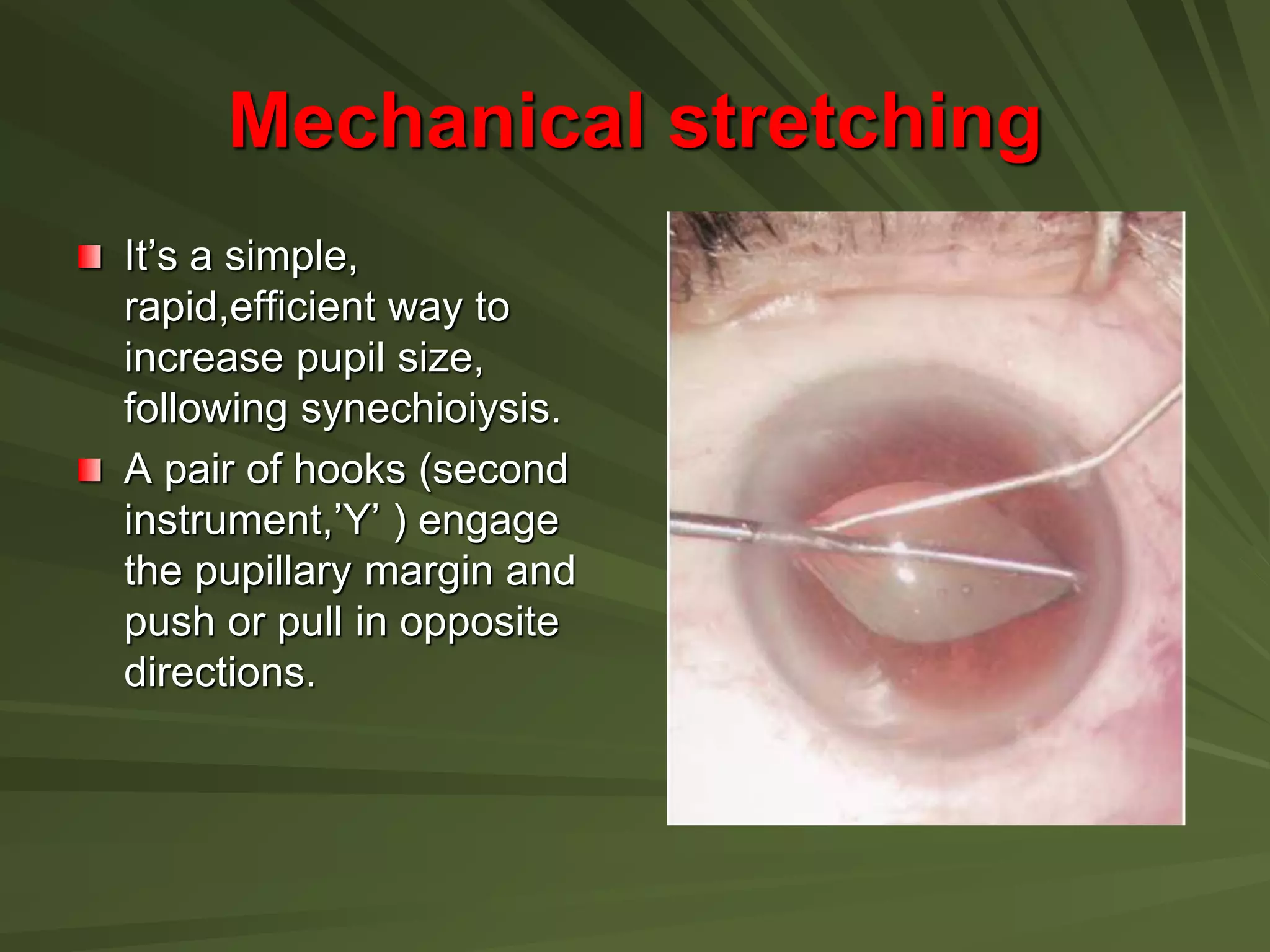
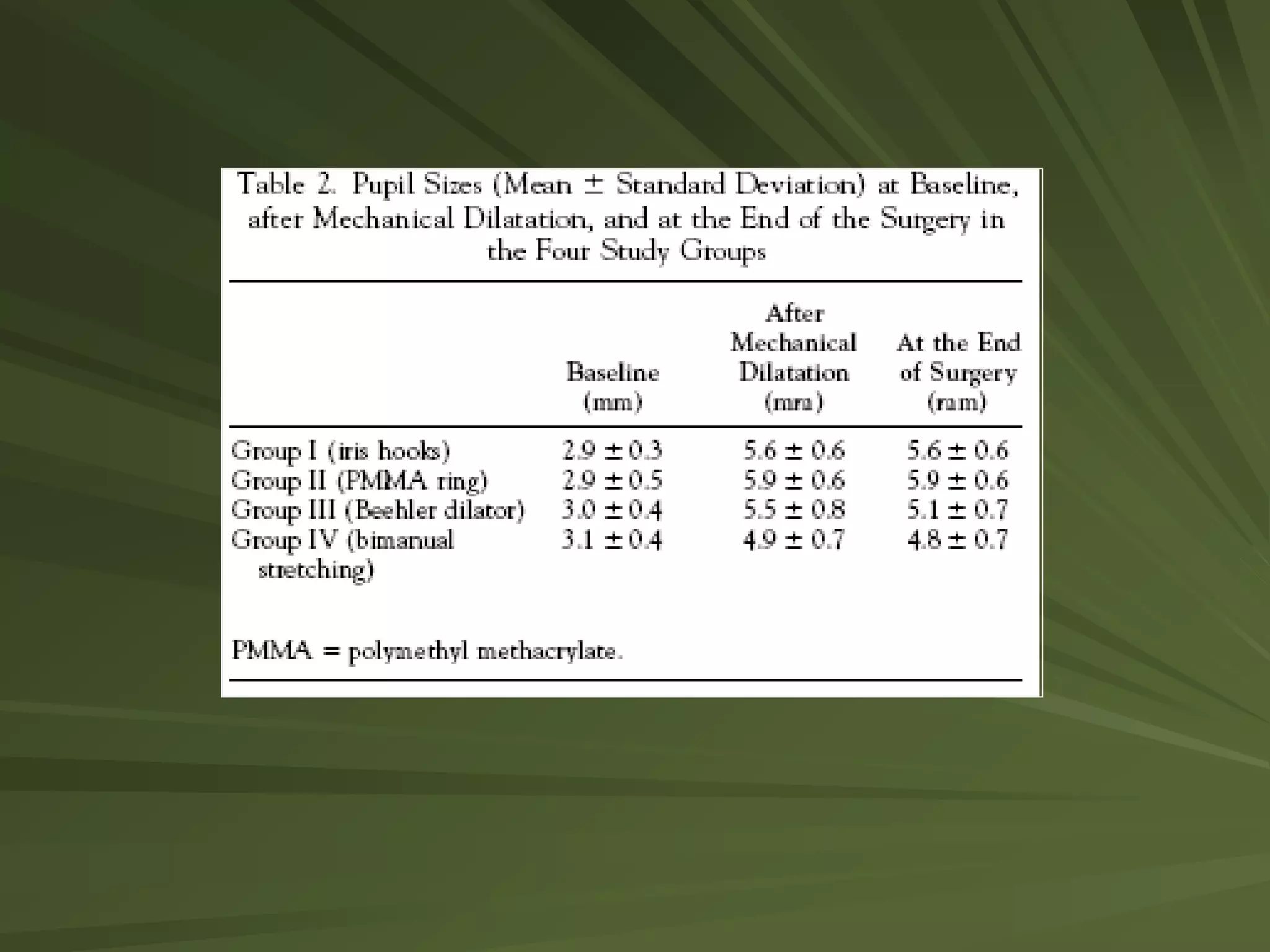
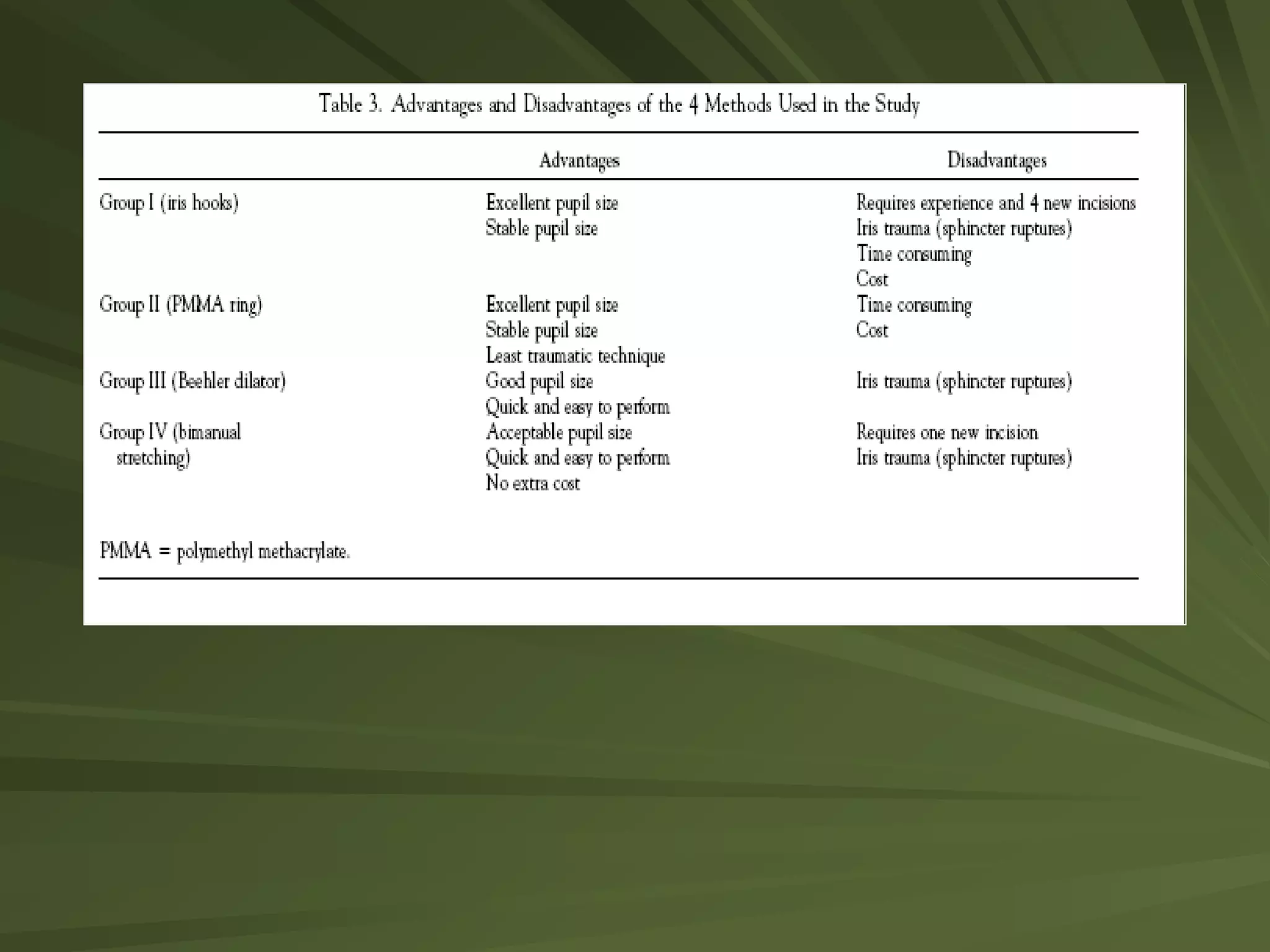
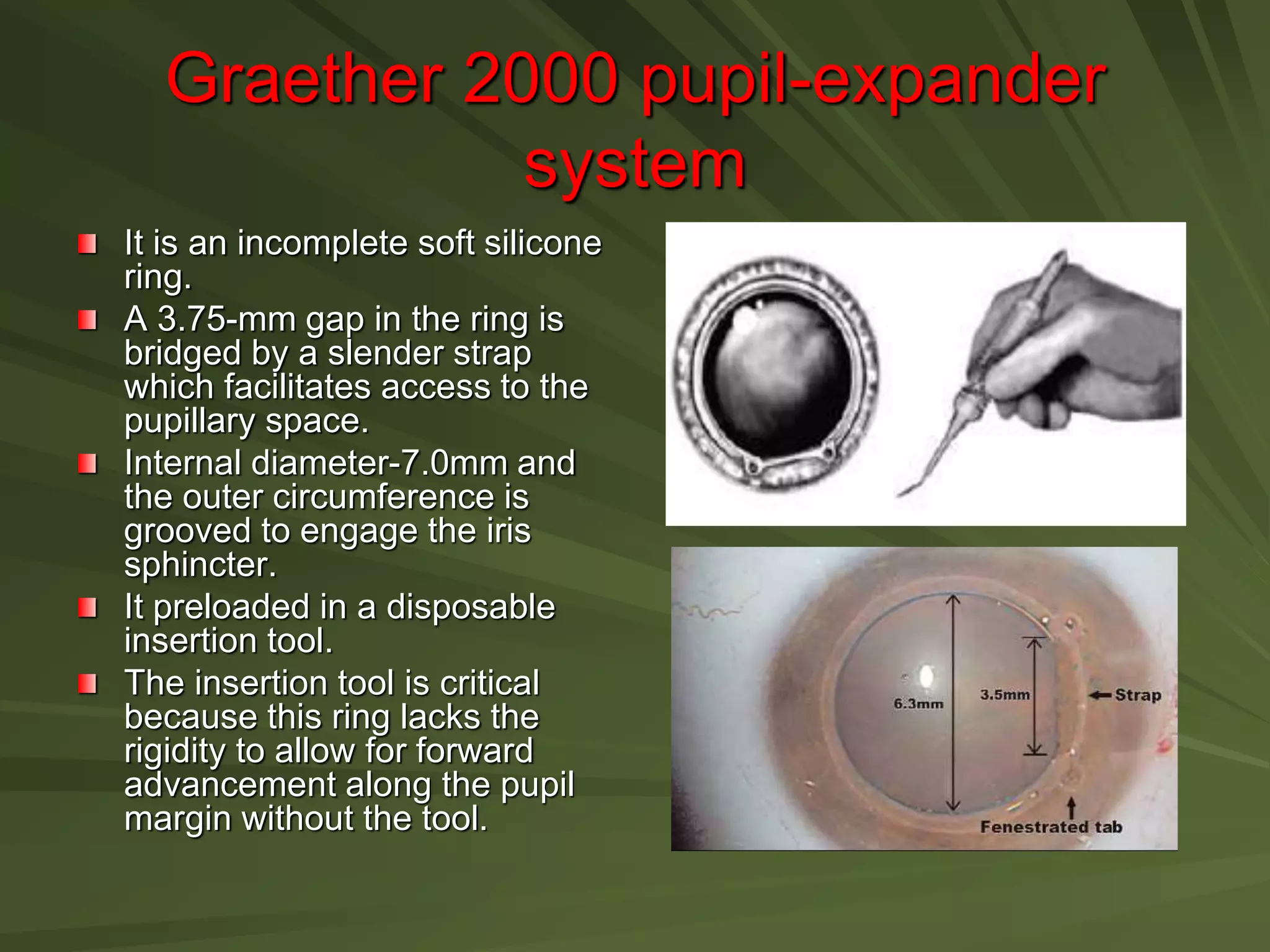
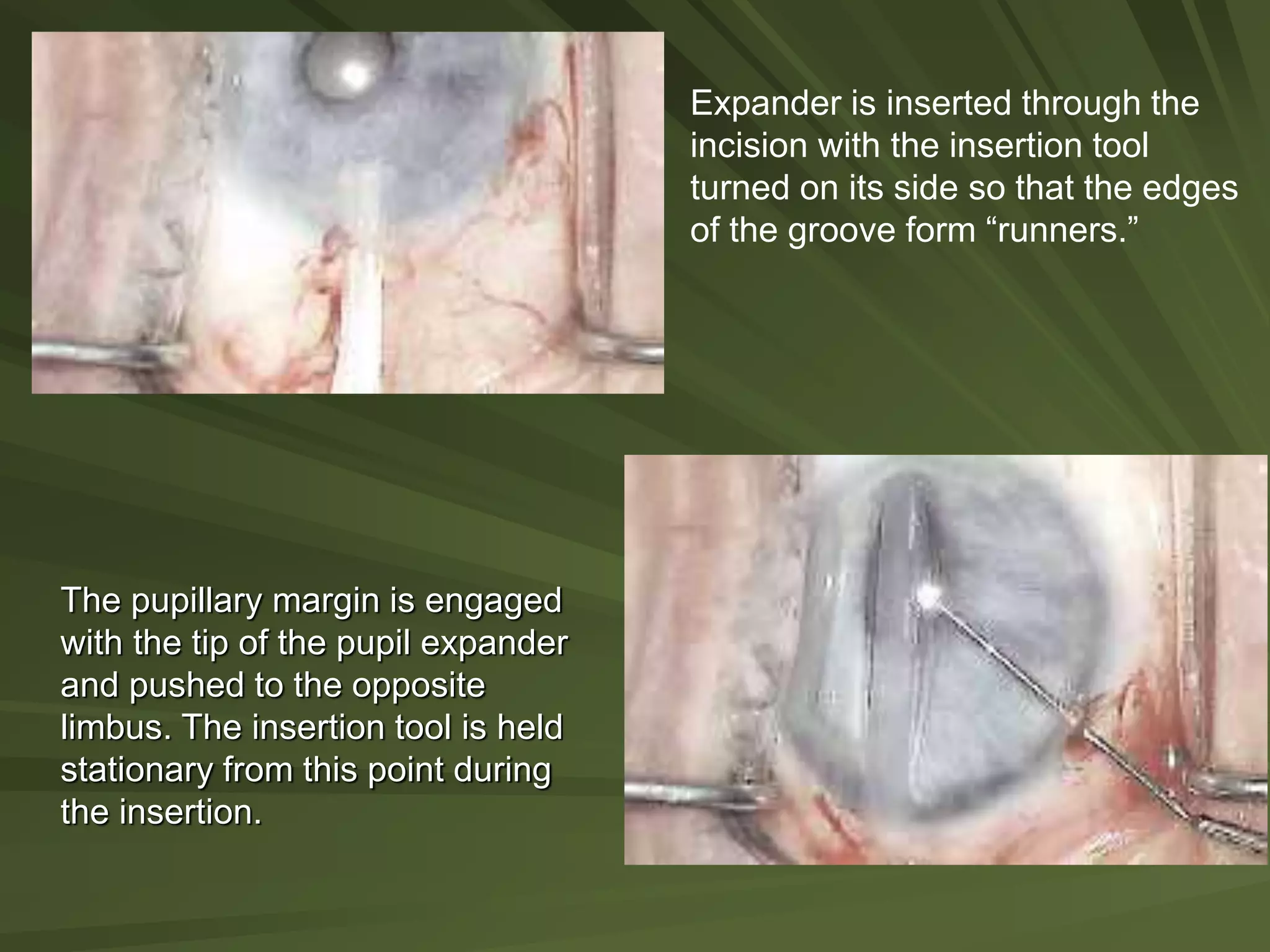
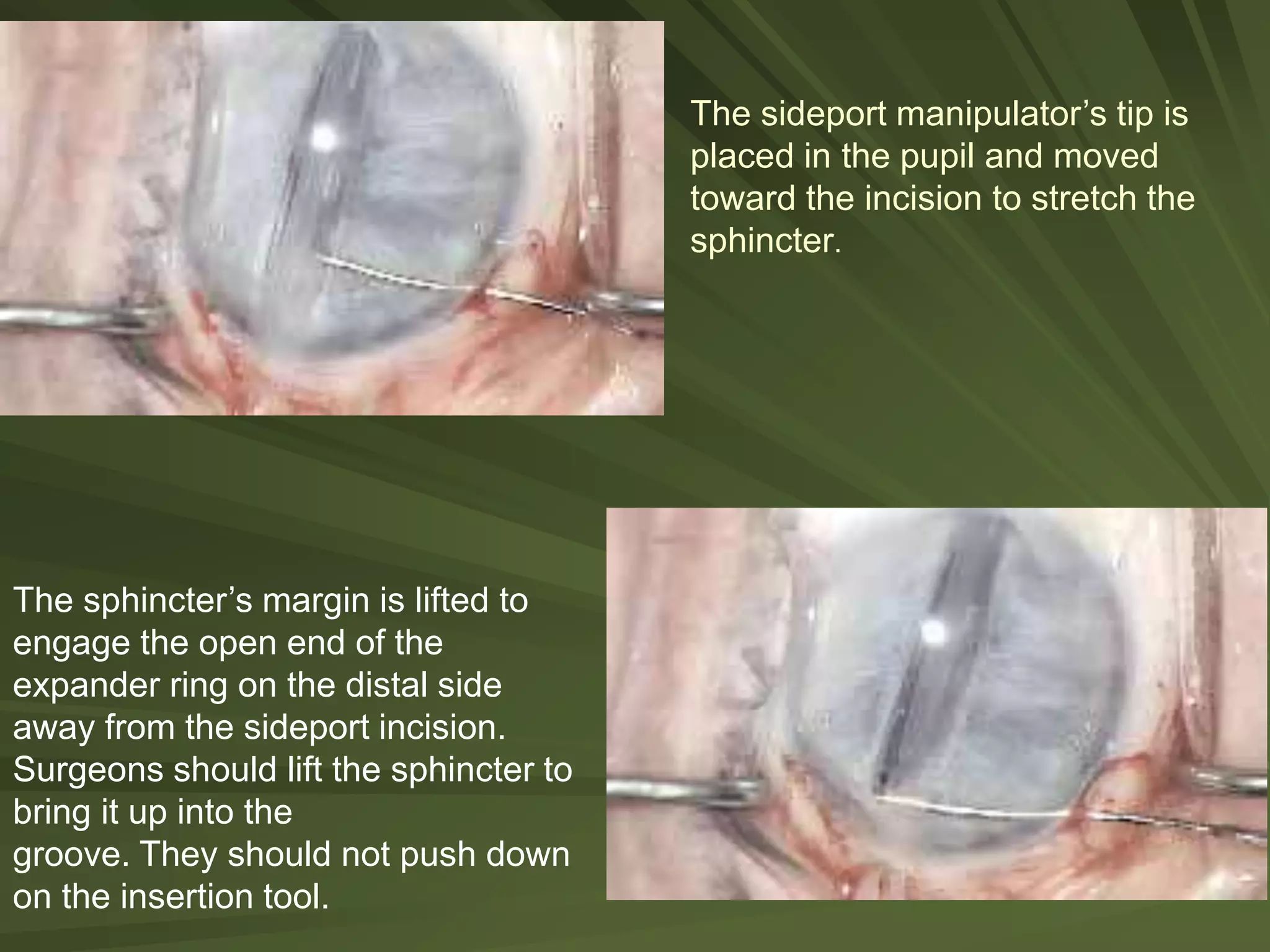
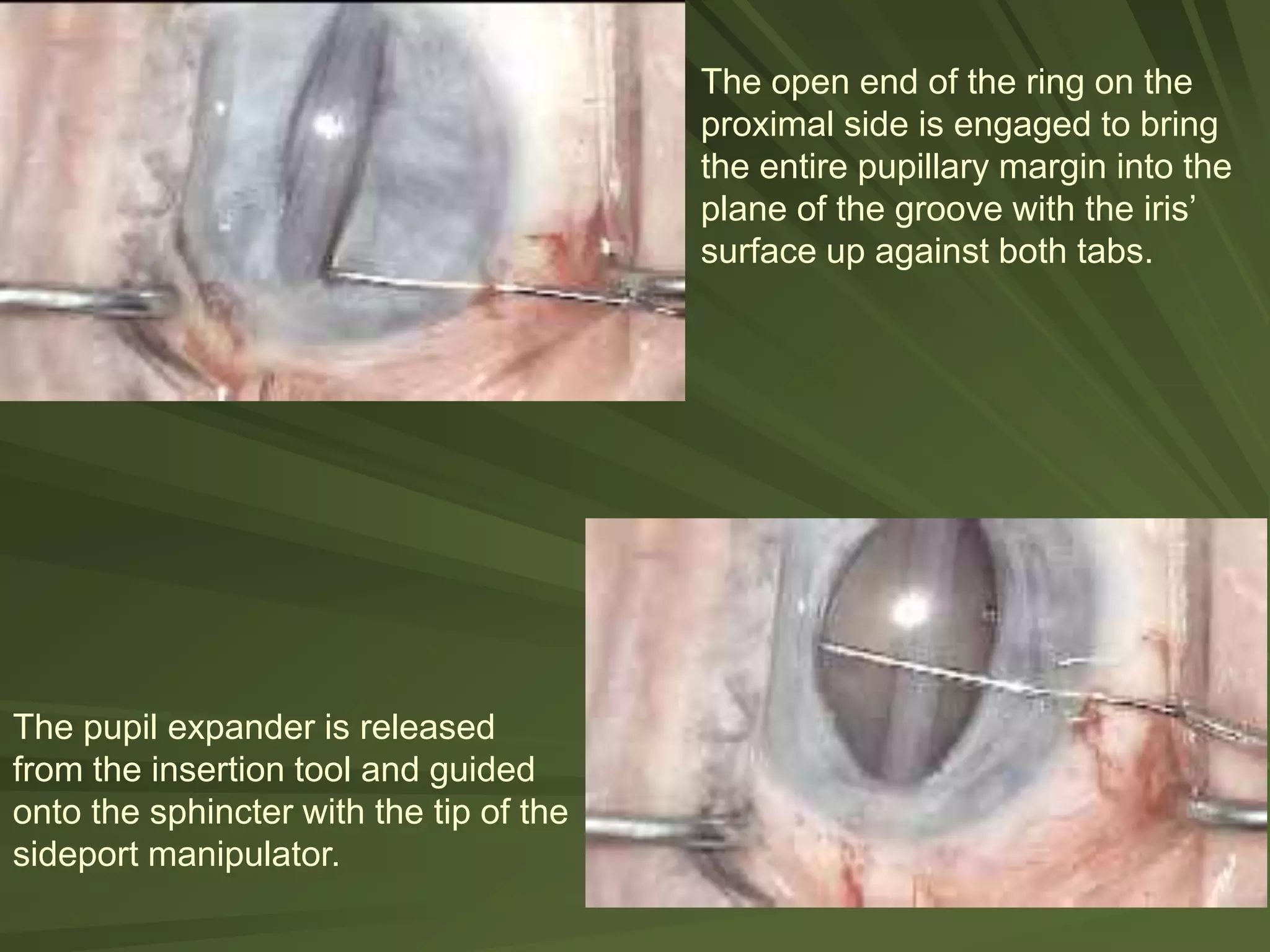
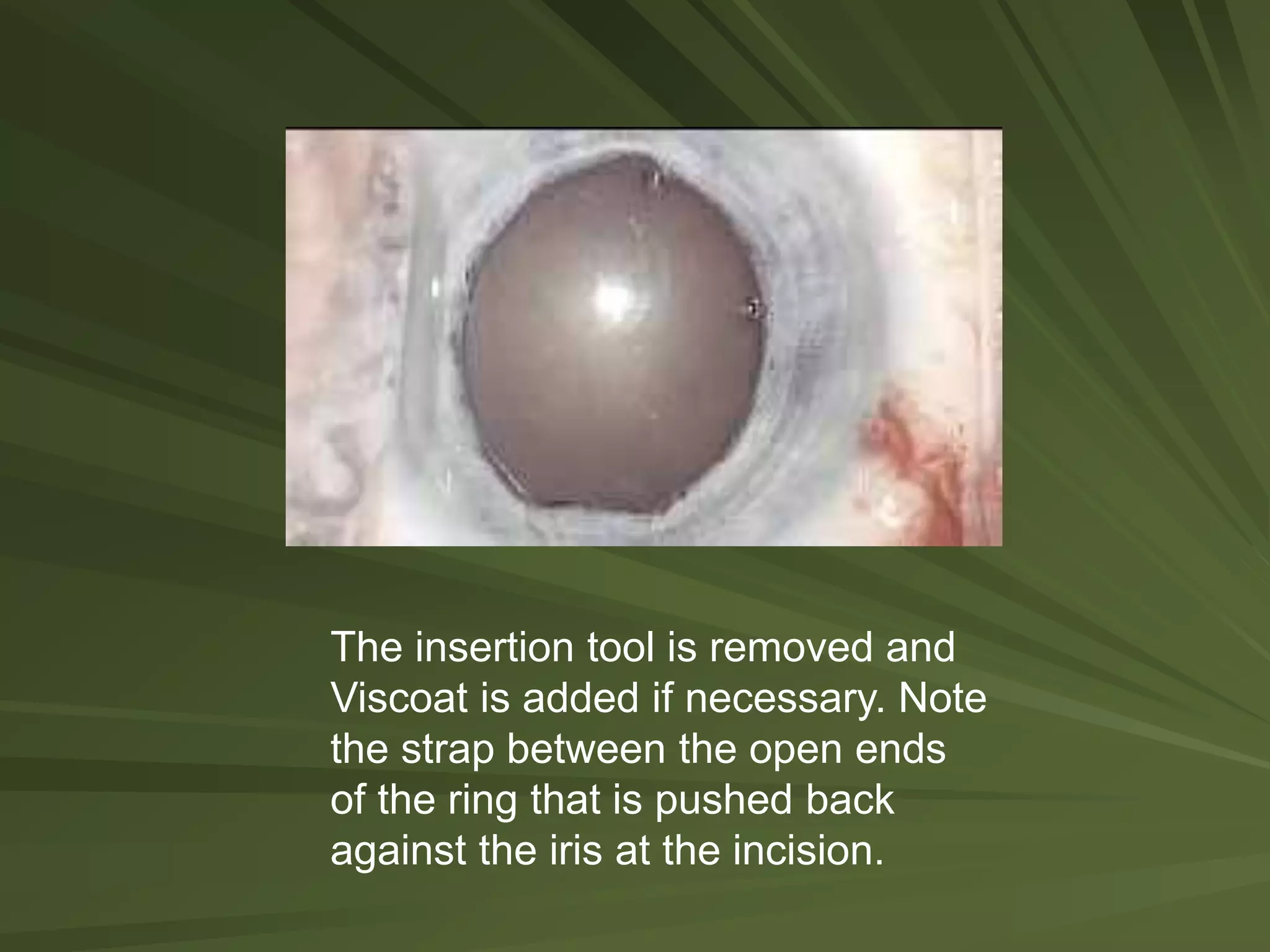
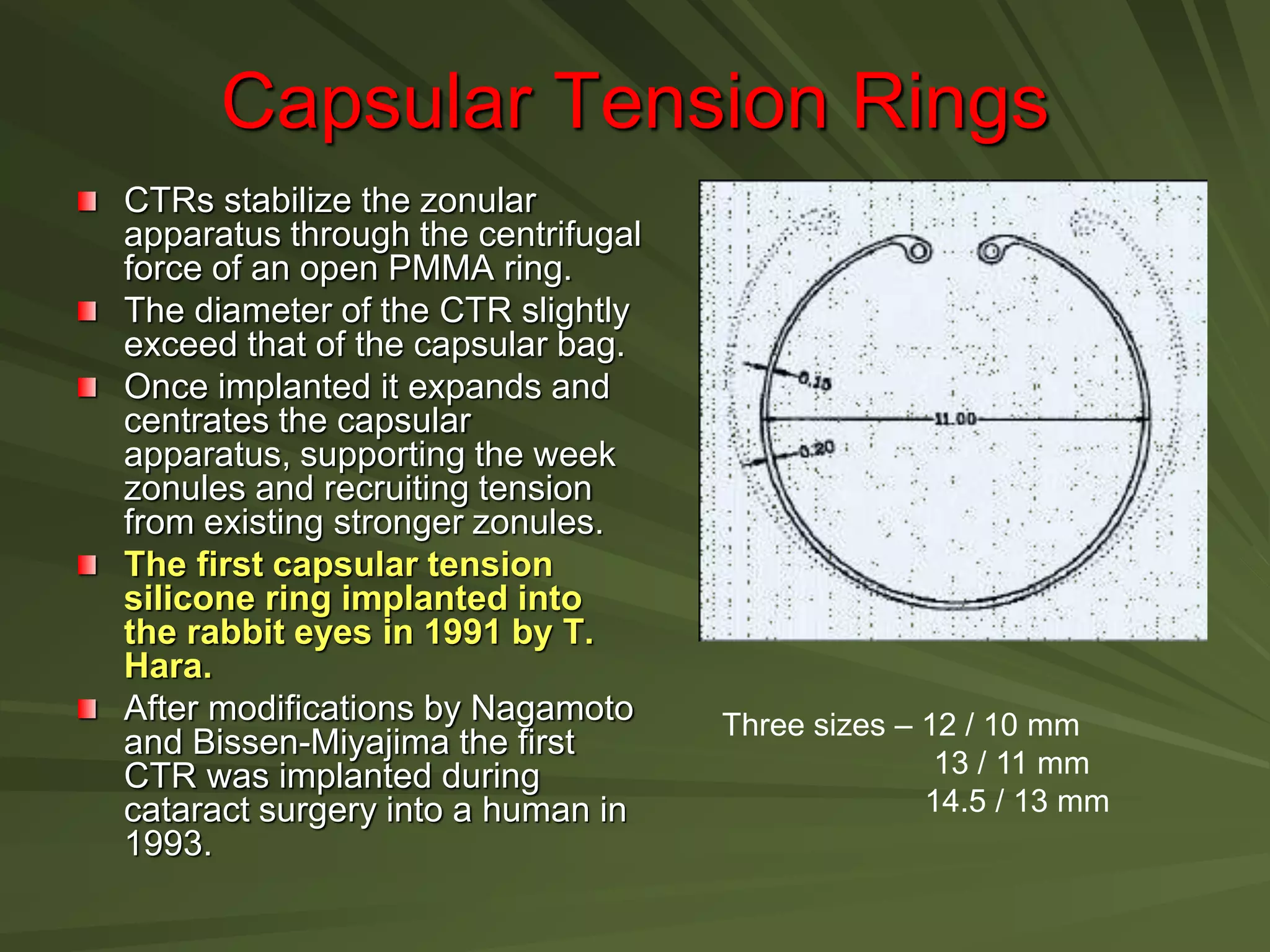
This document summarizes various adjunct devices used for pupil expansion and capsular stabilization during cataract surgery. It describes iris hooks, pupil stretchers, ring expanders, sodium hyaluronate, and iris sutures that can be used to increase pupil size in cases of inadequate dilation. It also discusses capsular tension rings and segments that provide support in cases of zonular weakness or instability to prevent complications. A study comparison found iris hooks and ring expanders produced the most stable pupil size but rings caused the least iris trauma. Overall, the document reviews indications and techniques for different intraoperative devices used to address operative challenges.










































![Ophthalmology INSTRUMENtS 2 [Autosaved]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/instruments2autosaved-1-240729155141-32d36116-thumbnail.jpg?width=640&height=640&fit=bounds)
























