

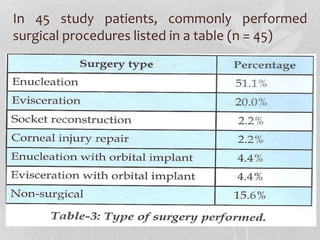
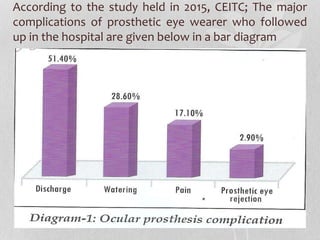
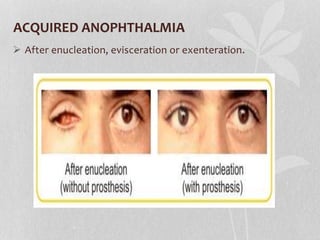
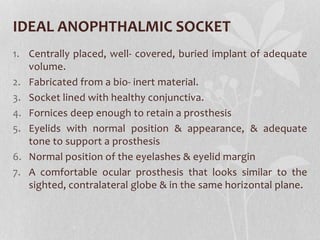
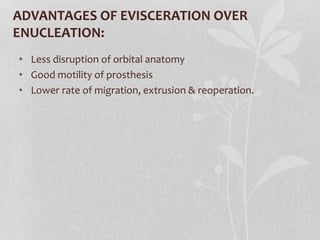

This document discusses ocular prosthetics and management of the anophthalmic socket. It begins by describing the surgical procedures of enucleation, evisceration, and exenteration used to partially or completely remove the eye. It then discusses goals and techniques after these surgeries, including the use of conformers and orbital implants. The document outlines fabrication of ocular prosthetics, including custom made versus ready made, and the impression fitting technique. Common complications are listed along with a study on complications. Ideal management is described to provide comprehensive eye care including prosthesis inspection and specialist referrals.














































![EYE REMOVAL TECHNIQUES [FINAL COPY BY FAITH KIMELI.] (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/eyeremovaltechniquesfinalcopybyfaithkimeli-250203210808-e559c479-thumbnail.jpg?width=640&height=640&fit=bounds)








![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











