Downloaded 435 times
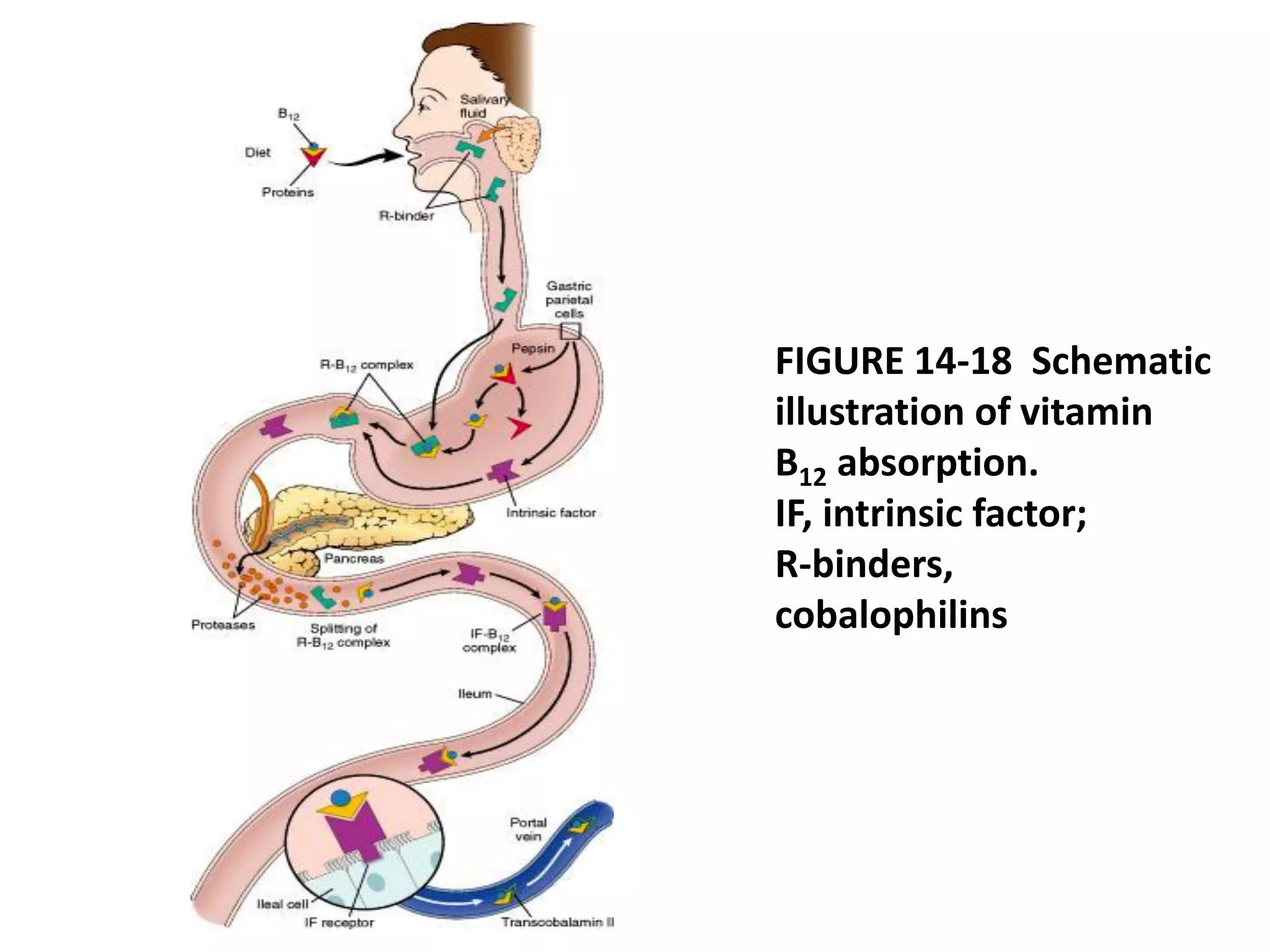

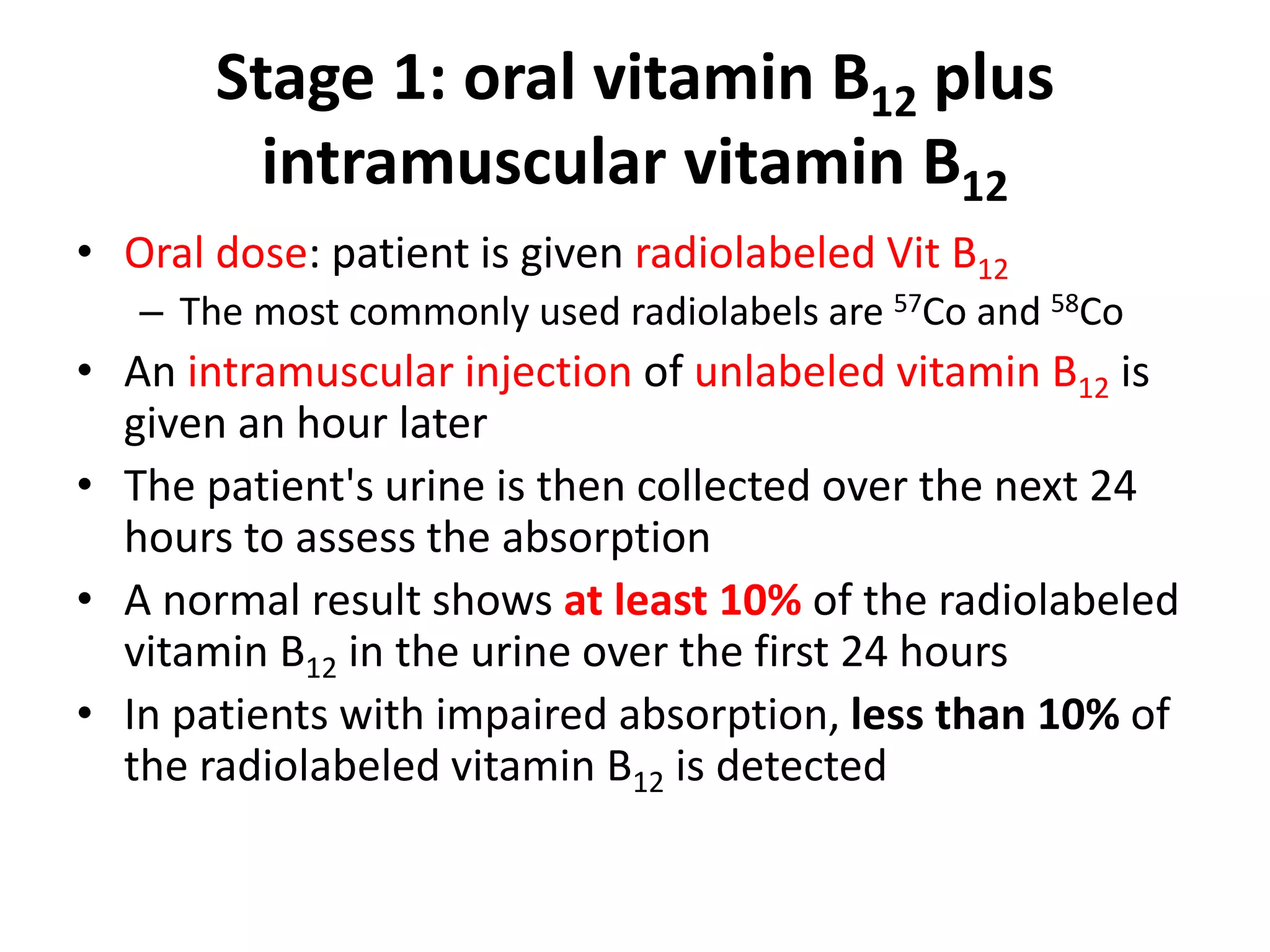
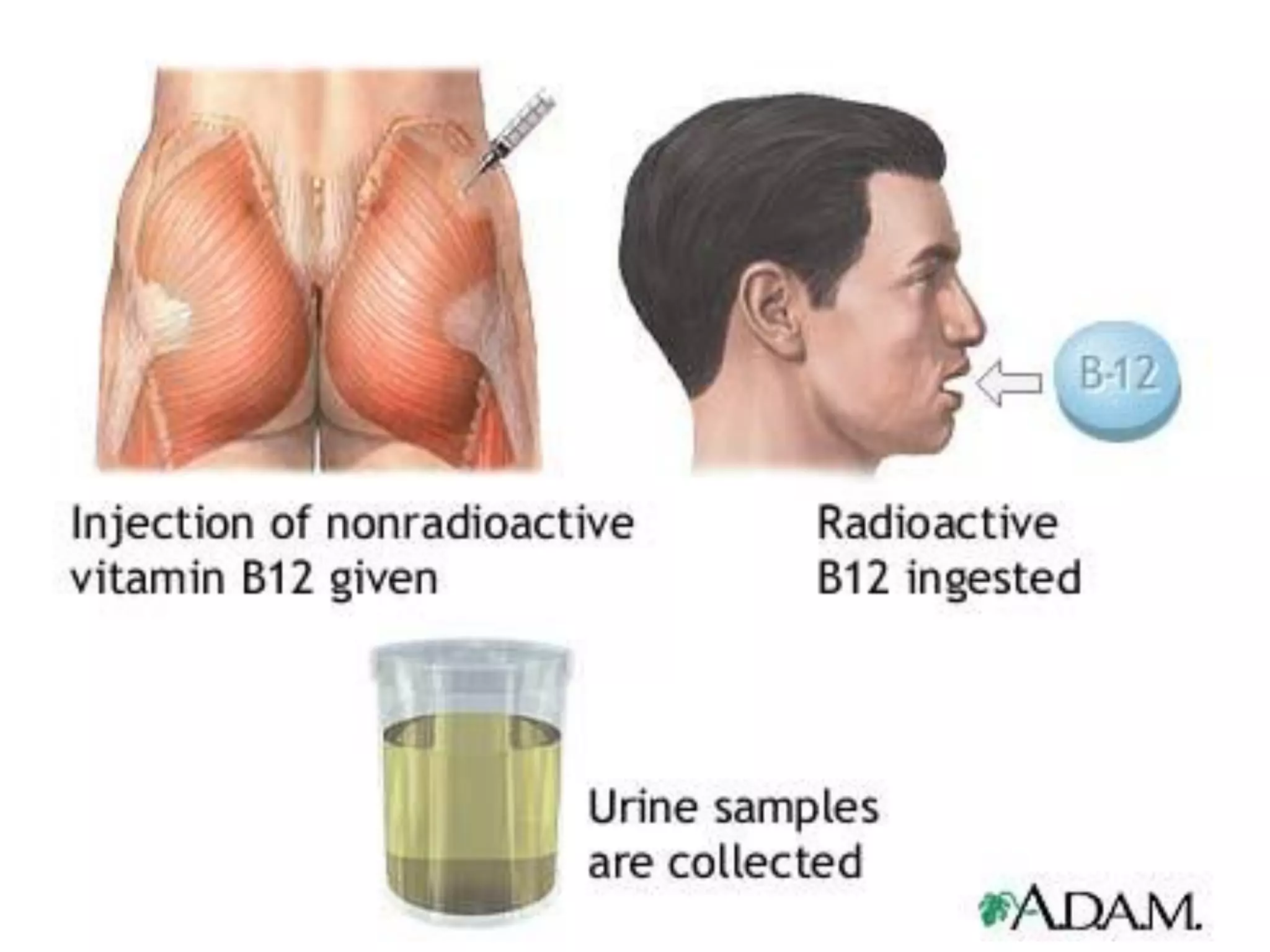















The Schilling test is used to evaluate vitamin B12 absorption in patients with vitamin B12 deficiency. It has multiple stages where radiolabeled vitamin B12 is given orally and/or intravenously along with intrinsic factor. Urine is collected to measure absorption. Abnormal absorption could indicate pernicious anemia from lack of intrinsic factor or other causes of malabsorption. The test helps differentiate these causes of vitamin B12 deficiency.


































































![[Int. med] anemia from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/8jbxzbhmt3ubllhnbjeg-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171706-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)







































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)
