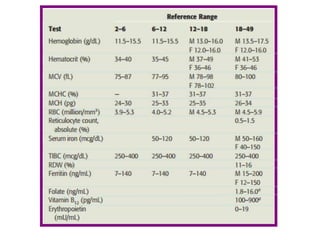
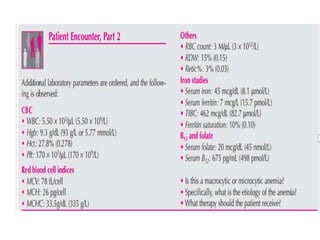
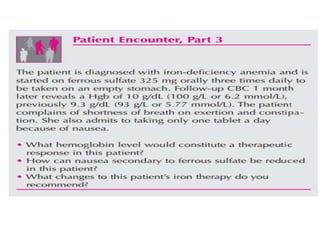
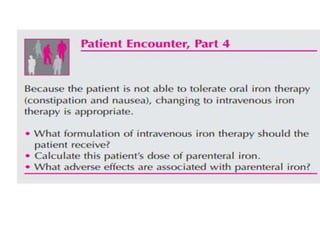
This document discusses anemia, including its definition, classification, symptoms, diagnosis, and treatment. Anemia is characterized by low hemoglobin and red blood cell counts, resulting in reduced oxygen-carrying capacity of blood. It is classified based on cell morphology, etiology, and pathophysiology. Common symptoms include fatigue, weakness, and shortness of breath. Diagnosis involves laboratory tests of hemoglobin, hematocrit, red blood cell indices, iron, vitamin B12, and folate levels. Treatment depends on the underlying cause, and may involve oral or intravenous iron supplementation for iron-deficiency anemia.































![Approach to Anemic Child [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtoanemicchildautosaved-240427131658-64d6d32d-thumbnail.jpg?width=640&height=640&fit=bounds)




































