Downloaded 124 times

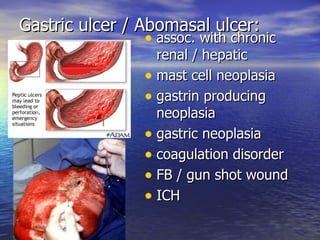
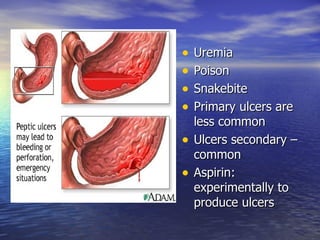
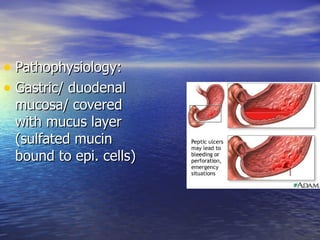
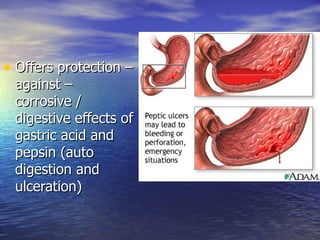

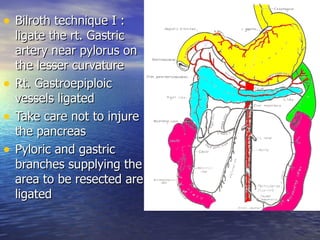

The document summarizes veterinary gastrointestinal surgery techniques for treating gastric ulcers. It discusses the causes, signs, diagnosis, and surgical treatment methods for gastric and abomasal ulcers in cattle and calves. The key surgical treatment discussed is the Bilroth I technique, which involves ligating blood vessels near the pylorus, excising the pyloric sphincter and canal, and anastomosing the gastric mucosa to the duodenum using absorbable sutures.






























































![STOMACH and DUODENUM SURGERY CLASS[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenumautosaved-250922162749-cdf69893-thumbnail.jpg?width=640&height=640&fit=bounds)




































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





