Downloaded 25 times
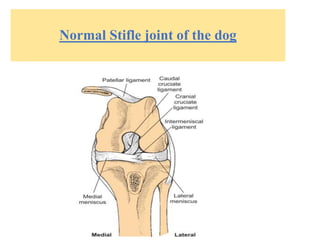
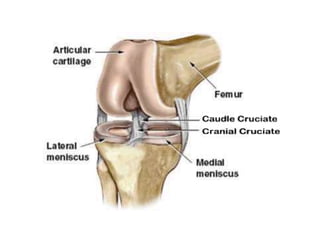
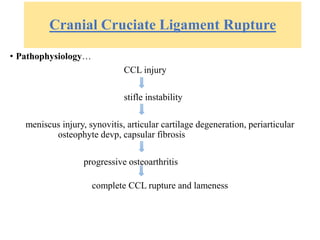
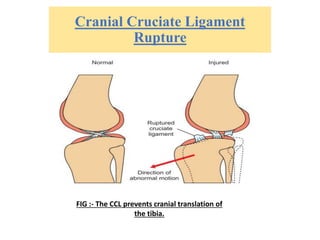
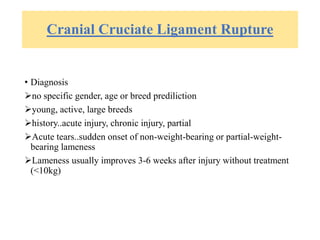
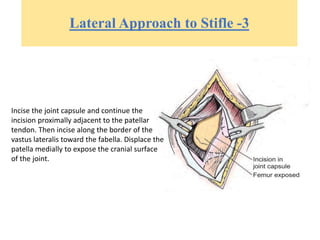







The document provides information on ligament injuries, specifically cranial cruciate ligament rupture in dogs. It discusses the pathophysiology, diagnosis, and treatment of cranial cruciate ligament rupture. Key points include: - The cranial cruciate ligament limits cranial translation of the tibia and controls internal rotation of the tibia. Rupture can be caused by traumatic injury or degeneration. - Diagnosis involves physical exam tests like the cranial drawer test and tibial compression test, as well as diagnostic imaging like radiography and arthroscopy. - Surgical treatment options aim to stabilize the stifle joint and include intracapsular reconstruction, extracapsular reconstruction, imbr