
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Gastrointestinal Veterinary Talk, Part 2
Similar to Gastrointestinal Veterinary Talk, Part 2 (20)
Recently uploaded
Recently uploaded (20)
Gastrointestinal Veterinary Talk, Part 2
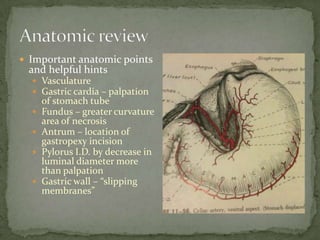
- 1. Important anatomic points and helpful hints Vasculature Gastric cardia – palpation of stomach tube Fundus – greater curvature area of necrosis Antrum – location of gastropexy incision Pylorus I.D. by decrease in luminal diameter more than palpation Gastric wall – “slipping membranes”
- 2. Proximal duodenum Duodenal papilla Major – bile duct and pancreatic duct Minor – accessory pancreatic duct
- 3. Proximal duodenum Duodenal papilla Major – bile duct and pancreatic duct Minor – accessory pancreatic duct
- 4. Proximal duodenum Duodenal papilla Major – bile duct and pancreatic duct Minor – accessory pancreatic duct
- 5. Duodenocolic ligament Holds distal descending duodenum to dorsal body wall Challenge to running bowel Easily transected if needed Difficult to suture adjacent duodenum if not transected
- 7. Full abdominal exploration - “Open them up” Be systematic Be gentle especially with linear foreign body
- 8. My approach Liver Stomach Duodenum and right pancreatic limb Right kidney and adrenal Jejunum, Ileum and Colon Left kidney and adrenal Bladder +/- Gall bladder expression +/- Opening omental bursa and left pancreatic limb
- 9. Surgical options Gastrotomy Gastropexy Gastrectomy Gastric resection anastomosis
- 10. Gastrotomy Location – ventral surface equidistance from greater and lesser curvature
- 11. Gastrotomy Minimize contamination Pack off abdomen Stay sutures Suction helpful Towel ready to receive what comes out Orogastric tube prior to entering lumen if fluid filled
- 12. Gastrotomy Minimize contamination Pack off abdomen Stay sutures Suction helpful Towel ready to receive what comes out Orogastric tube prior to enter lumen if fluid filled
- 13. Gastrotomy Stab incision Extend with scissors parallel to curvatures Separation of layers Mucosa-submucosa Muscularis-serosa
- 14. Gastrotomy Single or double layer closure I typically close in two layers using 3-0 PDS Mucosa-submucosa – simple continuous Serosa-muscularis – interrupted lembert No leak test The stomach wants to heal
- 15. Gastropexy Location Technique I only perform incisional 2-4 cm from pylorus Ventral midpoint of antrum Avoid lumen penetration Separation of layers +/- stay sutures
- 16. Gastropexy Location Technique Be aware of diaphragm = pneumothorax Glistening fascia Transverse incision not too dorsal Suture deepest to most superficial 2-0 PDS two continuous strands joined at most ventral aspect of pexy Avoid lumen penetration
- 18. Gastrectomy Indications Necrosis - GDV Neoplasia Ulcer with perforation Rupture
- 19. Gastrectomy Gastric viability Color Gray = bad Purple = likely OK Red = good Thickness Temperature Bleeding on cut serosal surface
- 20. Gastrectomy Technique Stapled – TA or GIA Cut and sew, cut and sew, etc. Lots of stay sutures Technically challenging Contamination Tissue thickness in intestinal forceps Invagination Serosa to serosa healing Easy No contamination
- 21. Gastric R-A Indications Neoplasia Perforating ulcer Hand sewn Single layer Complicated technically Lots of potential complications
- 22. Enterotomy and resection-anastomosis Appositional best Maintains luminal diameter Less fibrosis
- 23. Simple interrupted vs simple continuous Staples vs sutures Compendium 2000 Simple continuous better apposition Faster Staples – TA 35 (0.51 diameter close to 4.8mm x 3.4mm) Place 3 stay sutures and staples in between
- 24. What do I do? Ligaclips for vascular ligation Maintain as much mesoduodenum or mesojejunum as possible Suture terminal vessels
- 25. What do I do? SI with 3-0 or 4-0 PDS Take healthy bites 3-mm spacing Don’t worry about mucosal eversion unless severe Always leak test
- 26. Enterotomy Pack off to minimize contamination Surface to receive what is being removed Have everything ready Needle drivers Suture Thumb forceps Doyens or assistant No manipulation of vasculature
- 27. Enterotomy Longitudinal incision to transverse closure Increases luminal diameter Only used if small incision (i.e. biopsy) Generally not applicable at site of foreign body excision. Good for closure of site to cut string
- 28. BE GENTLE especially with small thread foreign bodies Typically hung in pylorus = gastrotomy Typically require multiple enterotomies Releasing and removing Minimize Critically evaluate viability Mesenteric border Duodenum adjacent to ligament Consider re-enforcements
- 29. Indications Intussusception Neoplasia Foreign body
- 30. Special considerations Contamination issues Gram neg. and anerobes Vasculature dissection more tedious Separation of layers Luminal disparity Oblique transection Variable tissue spacing Spatulation End-to-side
- 31. Special considerations Contamination issues Gram neg. and anerobes Vasculature dissection more tedious Separation of layers Luminal disparity Oblique transection Variable tissue spacing Spatulation End-to-side
- 32. Special considerations Contamination issues Gram neg. and anerobes Vasculature dissection more tedious Separation of layers Luminal disparity Oblique transection Variable tissue spacing Spatulation End-to-side
- 33. Indications Neoplasia Cecal inversion Technique Ileocecal and accessory cecocolic folds transected TA stapler very handy Simple interrupted
- 34. Indications Neoplasia Cecal inversion Technique Ileocecal and accessory cecocolic folds transected TA stapler very handy Simple interrupted
- 35. Indications Neoplasia Cecal inversion Technique Ileocecal and accessory cecocolic folds transected TA stapler very handy Simple interrupted
- 36. Indications Neoplasia Cecal inversion Technique Ileocecal and accessory cecocolic folds transected TA stapler very handy Simple interrupted
- 37. Closure re-enforcement Omentum Generally will attach without tacking. Tacking may speed up the process Serosal patching Time consuming I perform if I am worried
- 38. Closure re-enforcement Omentum Benefits Increased blood flow Rapid fibrin seal Generally will attach without tacking. Tacking may speed up the process Serosal patching Time consuming I perform if worried
- 39. Nutritional support Jejunostomy tube
- 40. Explore again to make sure Full thickness BIOPSY Stomach Duodenum and jejunum 4-mm skin punch biopsy (+/-) Ileum Don’t biopsy colon unless essential
- 41. Lavage Warm saline in water bath or microwave 200-300 ml/kg I use: Small dogs and cats – 1-2 liters Medium dogs – 2-3 liters Large dogs – 4-6 liters Keep flushing until clear Remove blood clots
Editor's Notes
- Compendium 2000Author – Bradley CoolmanSimple continuous better appositionFasterStaples – TA 35 (0.51 diameter close to 4.8mm x 3.4mm)Place 3 stay sutures and staples in between
- LavageWarm water bath200-300ml/kg recommended. We typically use:1-2 liters – small dogs and cats2-3 liters – medium dogs4-6 liters – large dogsKeep flushing until fluid is clear, no active bleeding and all blood clots removed. Contaminated fluid left in the abdomen can complicate healing process especially if associated with significant volumes of blood or bile.