Downloaded 166 times

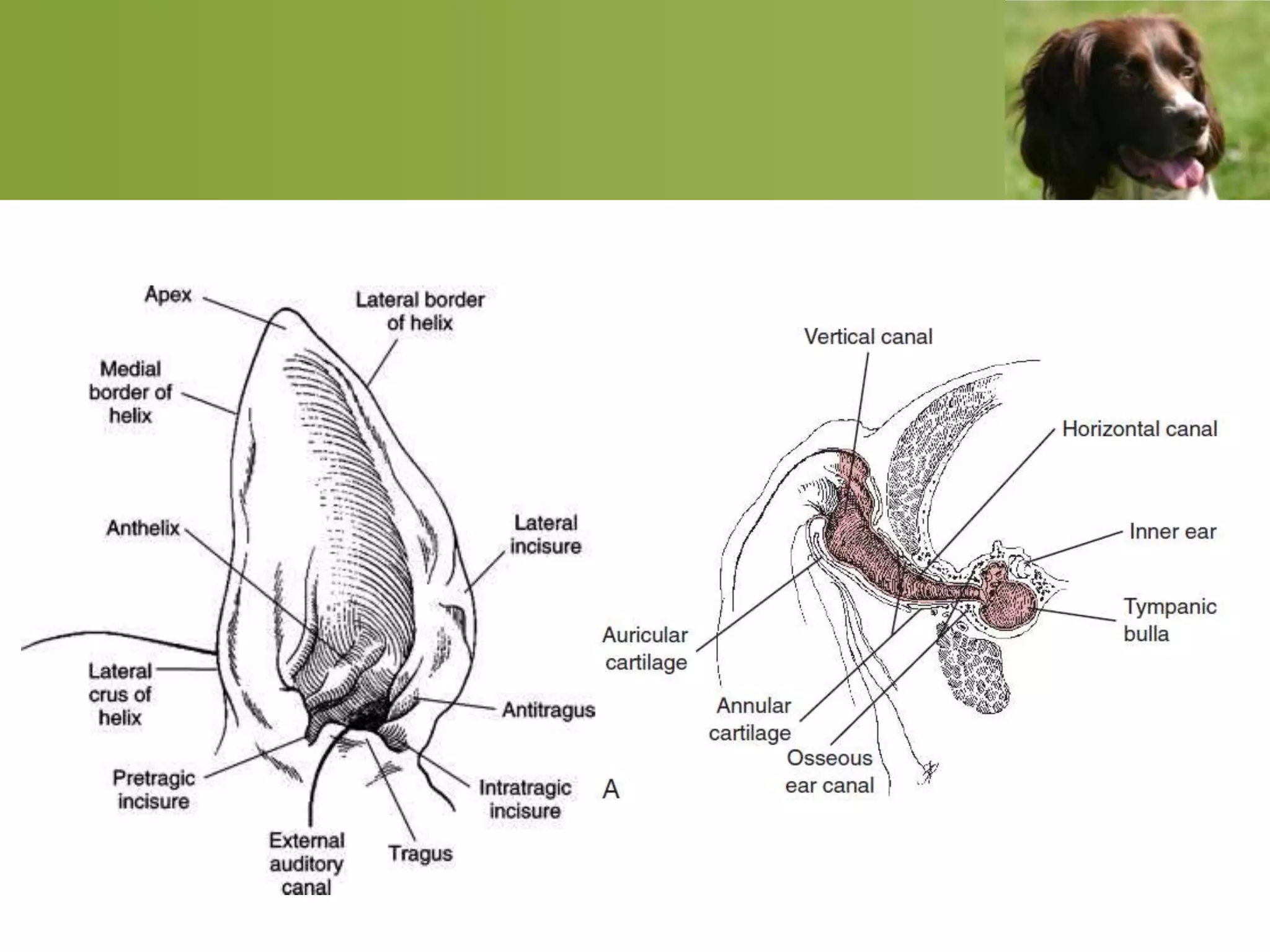









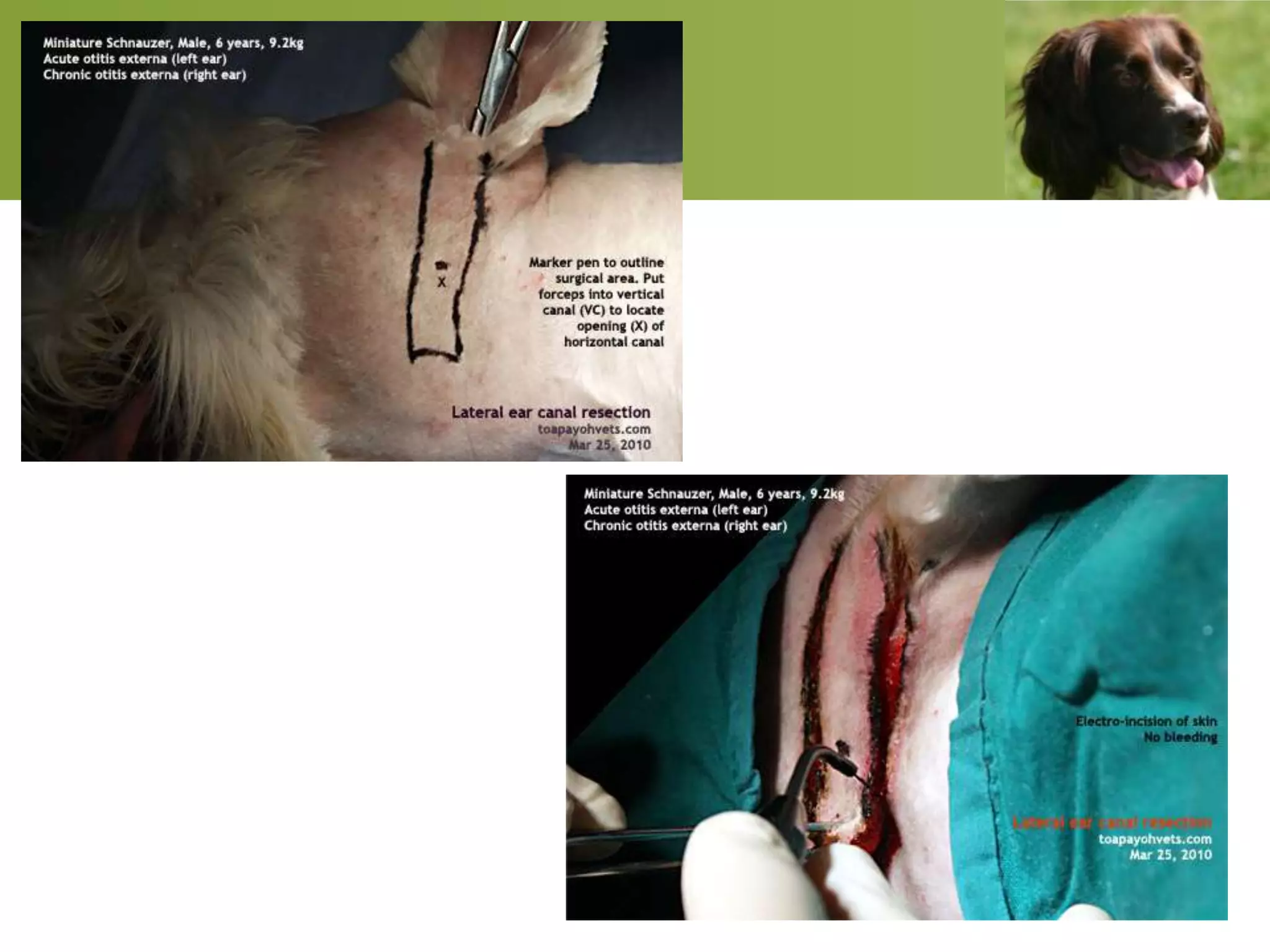





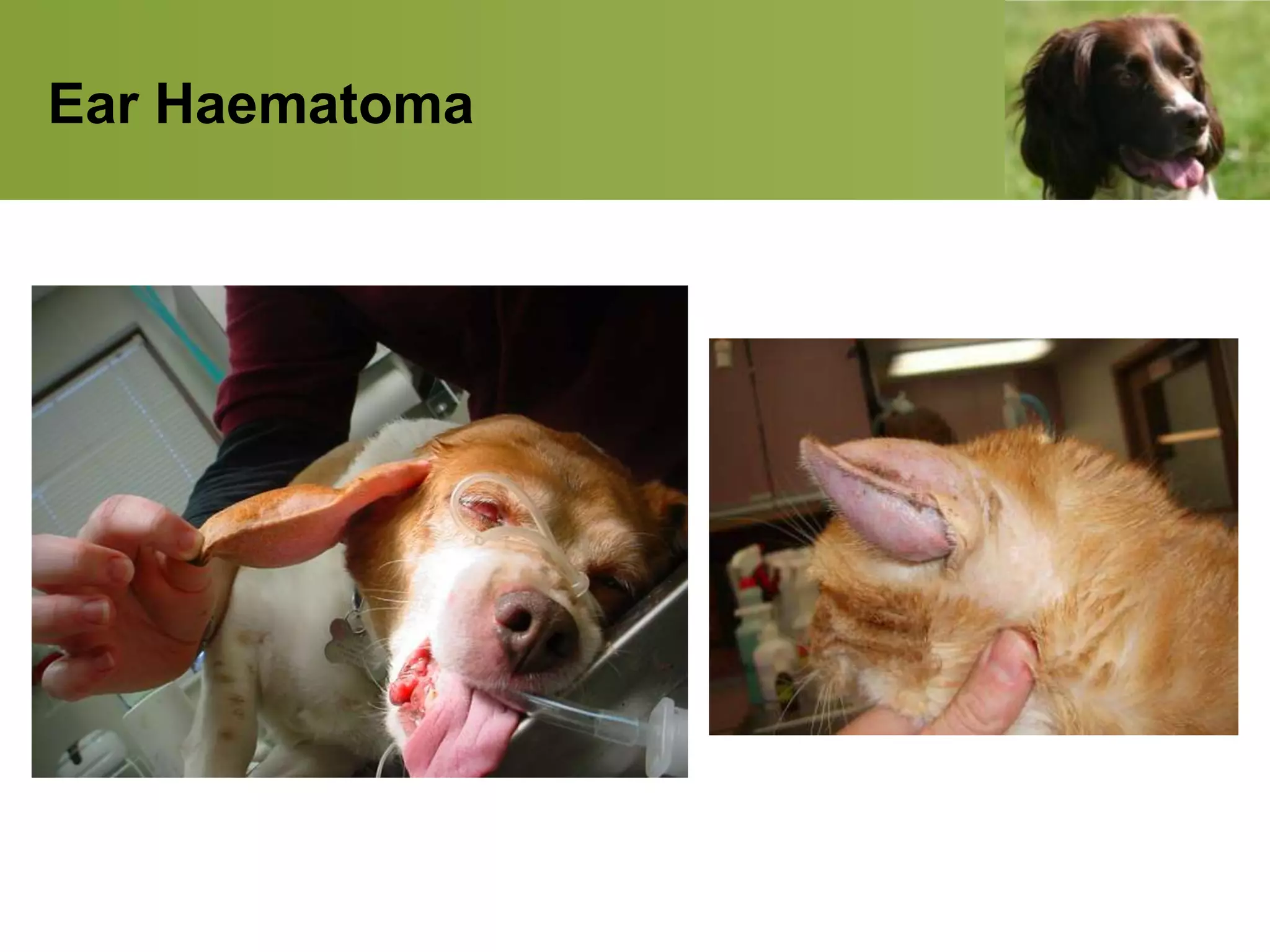


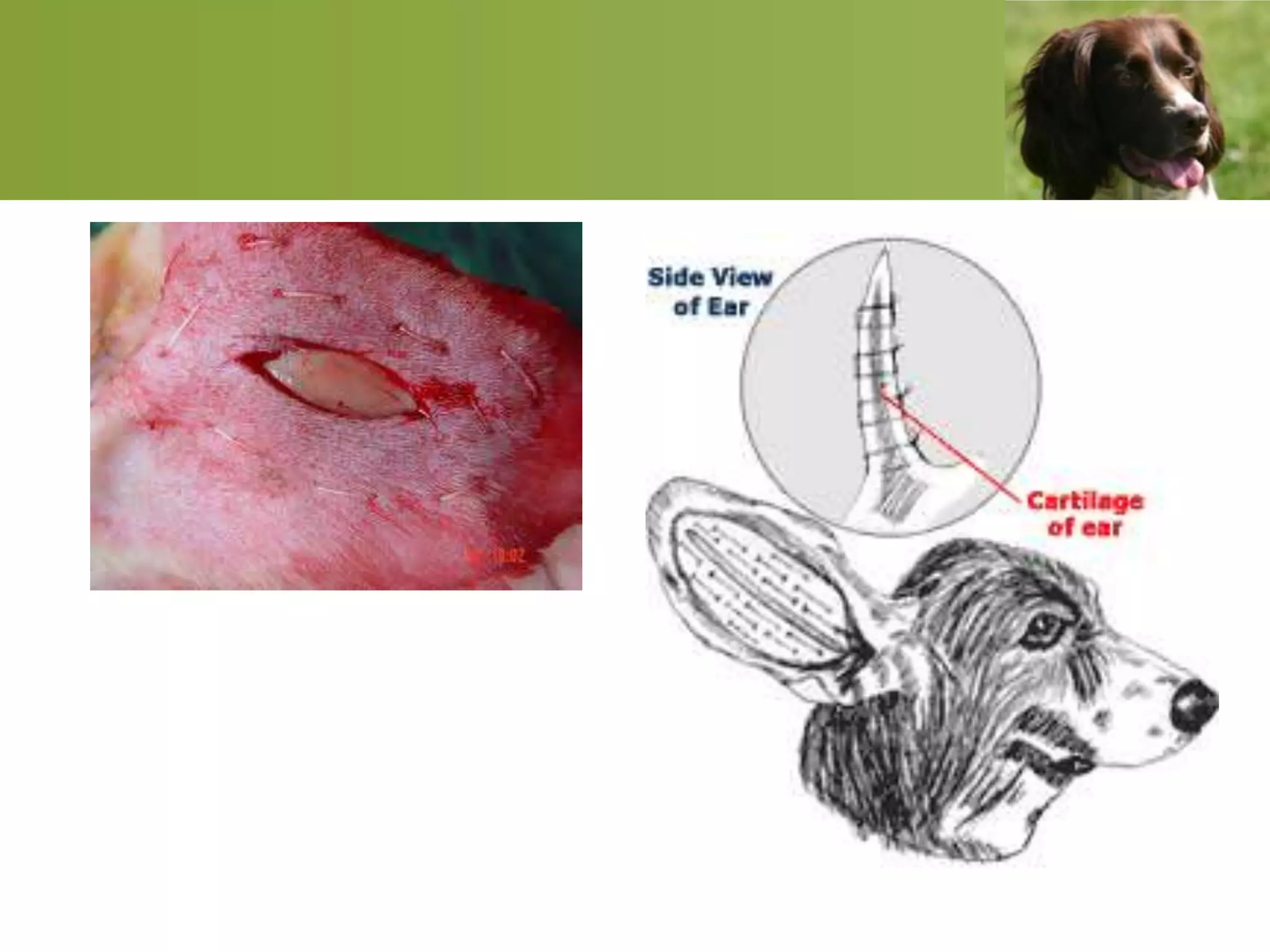







This document discusses ear conditions in pets. It covers otitis externa (inflammation of the outer ear), including common signs like head shaking and discharge. Otoscopic examination of the ear canal is described. Treatment for otitis externa involves cleaning and applying medications to the ear canal. Other conditions covered include auricular hematoma, otitis media (middle ear inflammation), and otitis interna (inner ear). Surgical techniques like lateral ear canal resection are discussed. Diagnosis and treatment of otitis media and interna involve cytology, antibiotics, and anti-fungals based on culture results from the infected areas.























































































