Downloaded 213 times

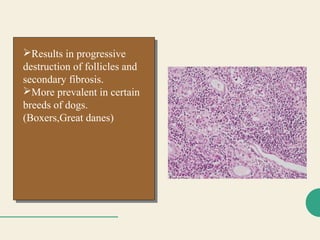





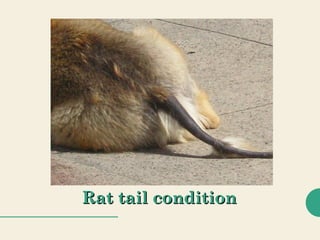
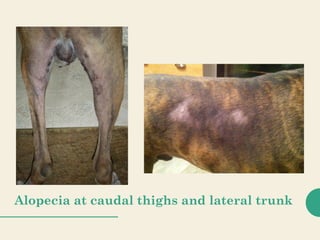
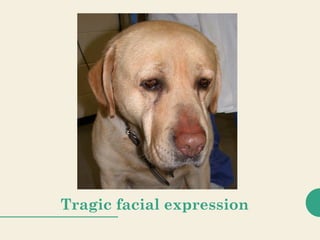


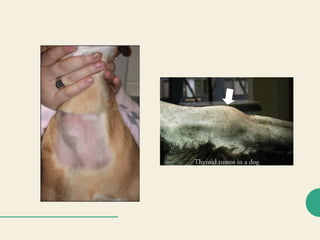

Hypothyroidism and hyperthyroidism in dogs are endocrine diseases caused by impaired or excessive thyroid hormone production respectively. Hypothyroidism is more common and seen as lethargy, weight gain, hair loss, and other metabolic signs. It is diagnosed via low thyroid hormone levels and treated with levothyroxine supplementation. Hyperthyroidism is rare in dogs and caused by functional thyroid tumors, seen as weight loss and other hypermetabolic signs.




























![1525488865092_presented_Credit_seminar_canine_hypothyroidism[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/1525488865092presentedcreditseminarcaninehypothyroidism1-230203135630-25164c14-thumbnail.jpg?width=640&height=640&fit=bounds)















































