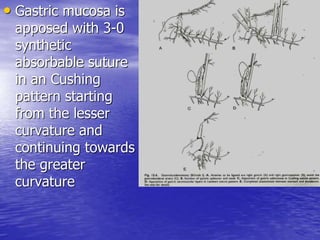
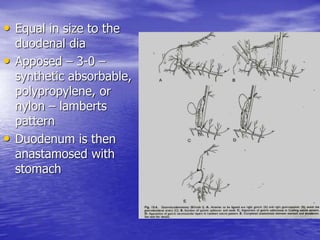
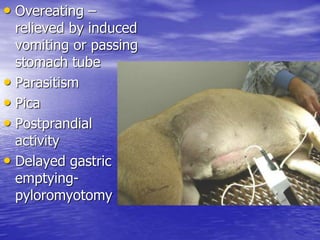
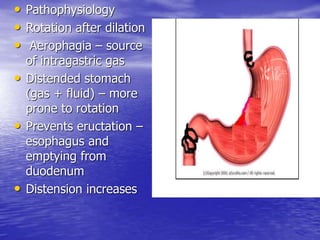
This document discusses various gastrointestinal surgical procedures in veterinary medicine. It covers topics such as gastric and abomasal ulcers, gastric dilatation and torsion, gastric neoplasms, bloat, and rumen fistulation and rumenotomy. Diagnostic techniques including radiography, endoscopy, and ultrasound are mentioned. Surgical treatments including gastrectomy, pyloroplasty, and rumenostomy are summarized. The document provides an overview of common gastrointestinal surgical conditions and procedures in large animals.















![STOMACH and DUODENUM SURGERY CLASS[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/stomachandduodenumautosaved-250922162749-cdf69893-thumbnail.jpg?width=640&height=640&fit=bounds)







































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




