Downloaded 39 times



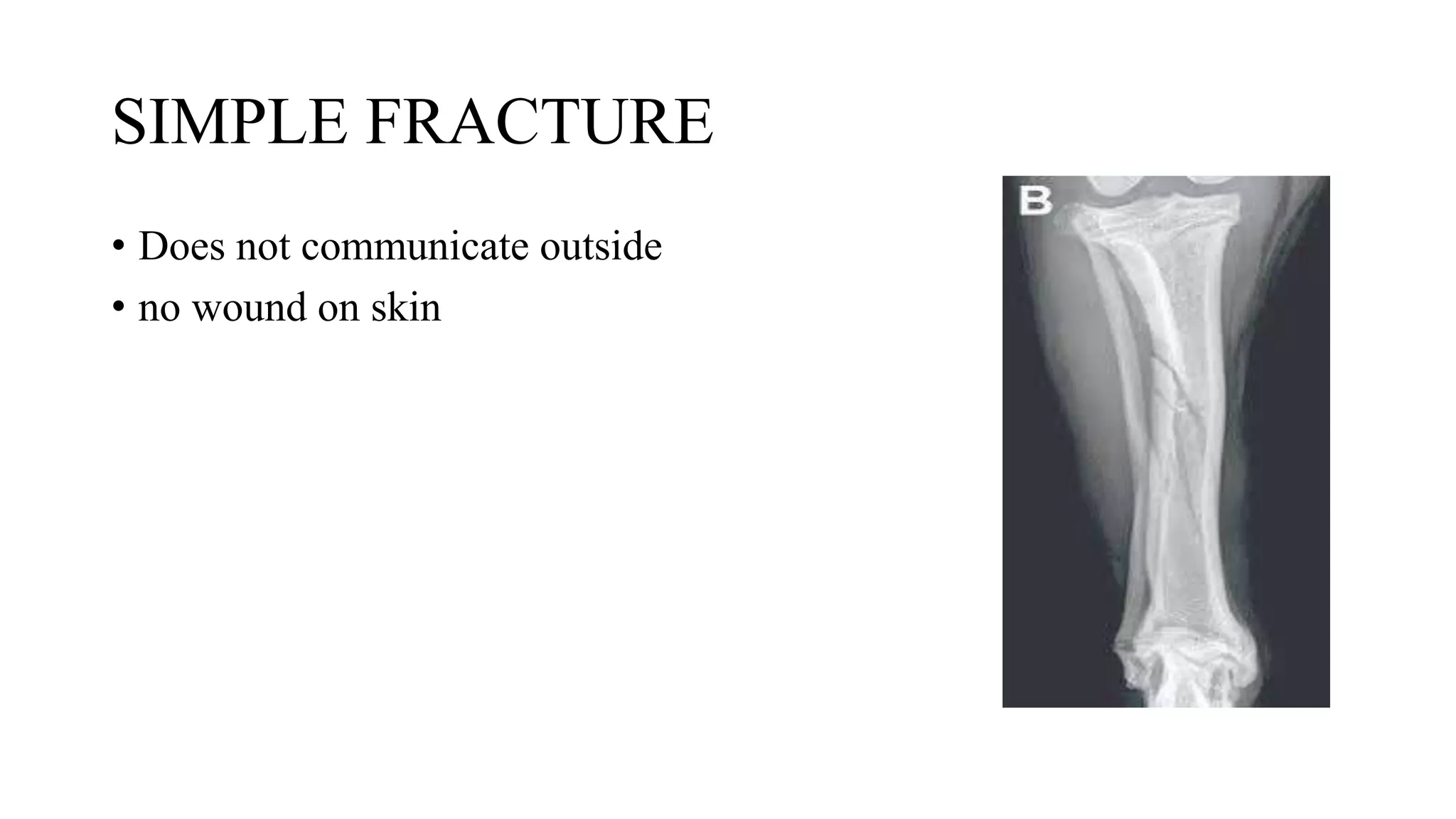







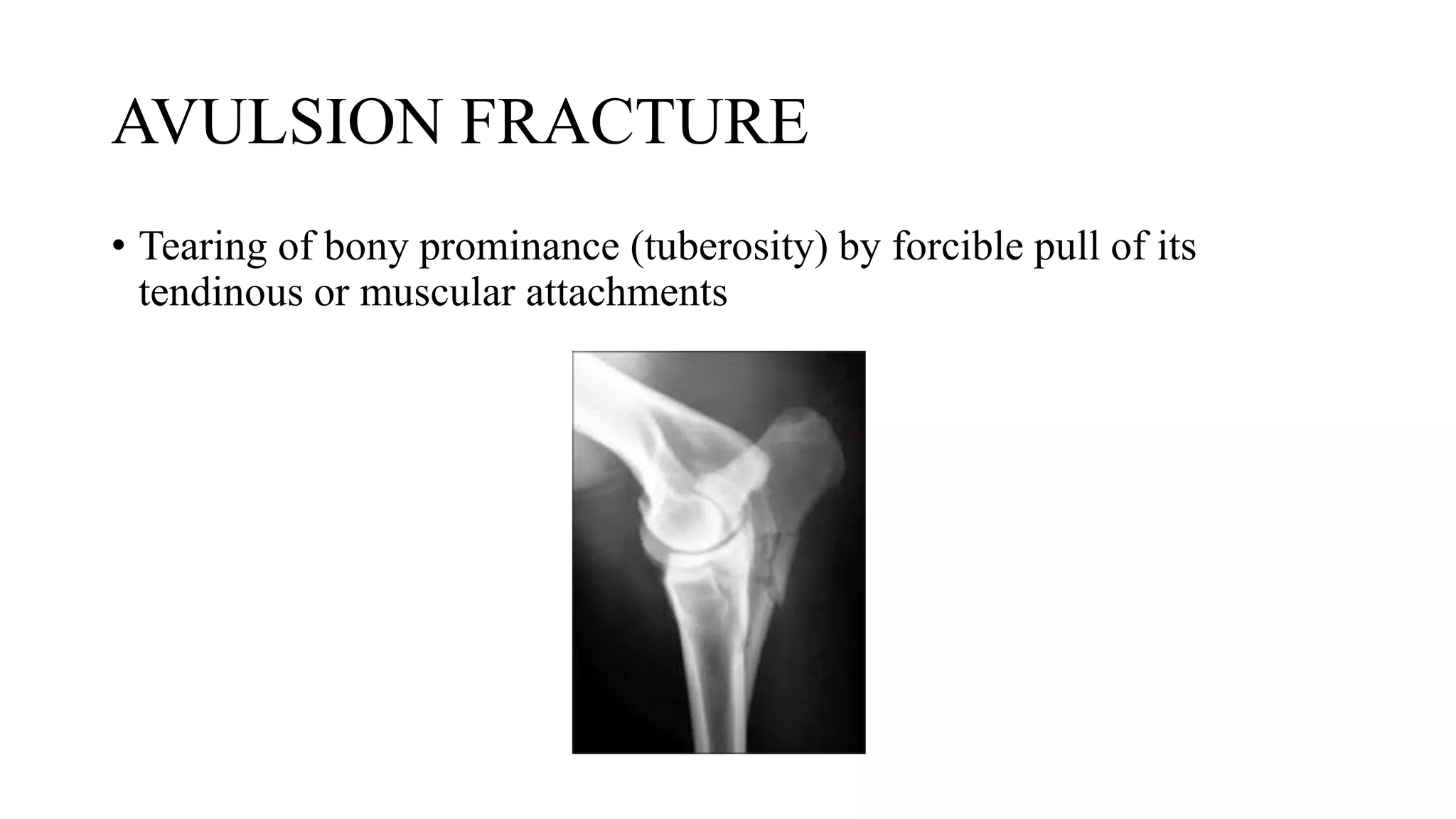





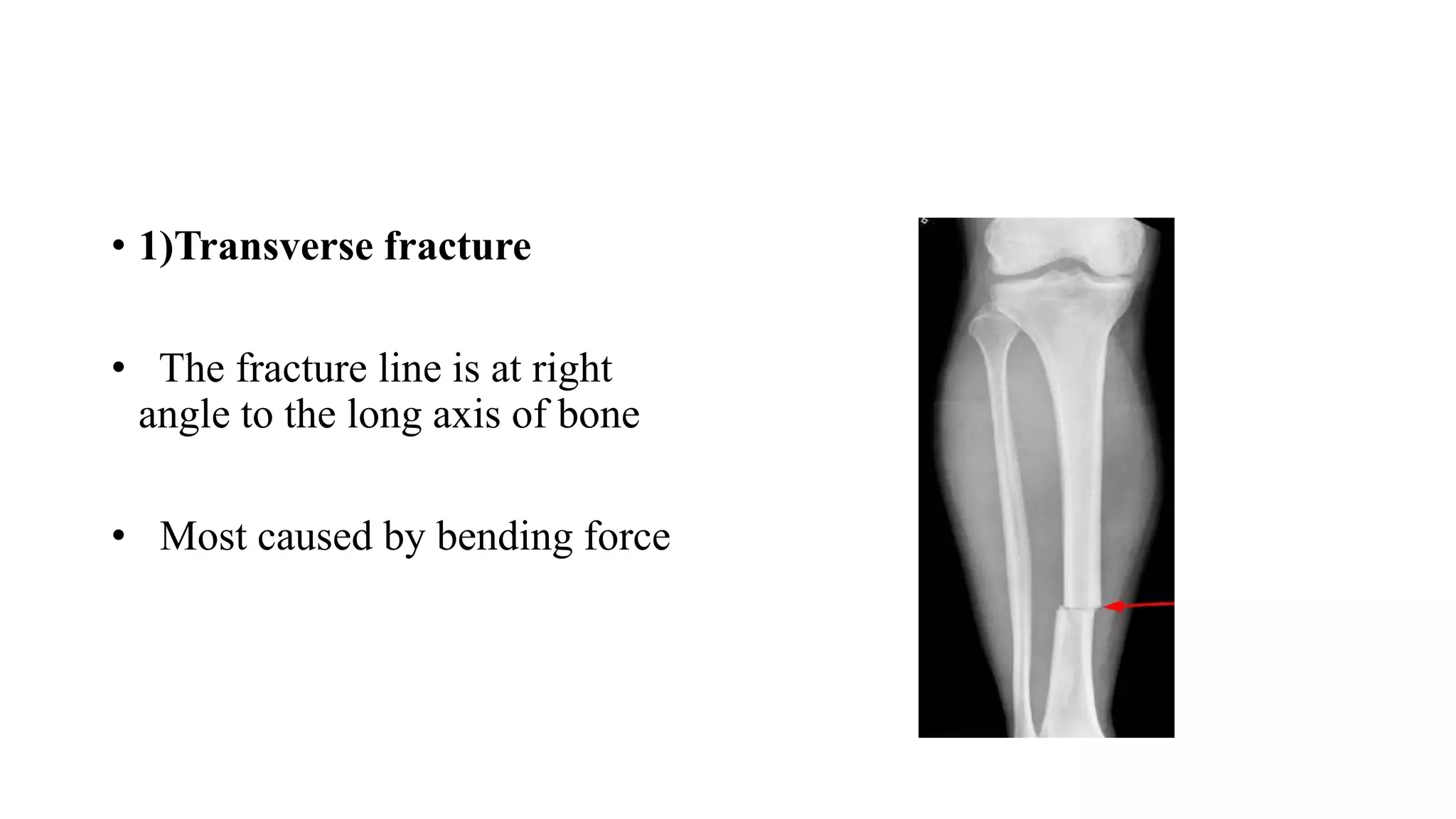
































This document discusses the classification of fractures in veterinary medicine. It defines a fracture as a break in bone continuity and classifies fractures based on several factors, such as simplicity, completeness, location, displacement of fragments, soft tissue involvement, and bone affected. Common types of fractures described include simple, compound, incomplete, complete, avulsion, complicated, greenstick, and comminuted fractures. Diagnosis involves clinical examination findings as well as radiography, bone scans, CT, micro CT, and MRI. Classification systems provide a standardized way to describe fractures aiding in prognosis and treatment planning.