Tetrology of fallot
•Download as PPT, PDF•
46 likes•9,808 views

Tetralogy of Fallot is a congenital heart defect with four abnormalities: 1) a ventricular septal defect, 2) pulmonary stenosis, 3) overriding aorta, and 4) right ventricular hypertrophy. This causes deoxygenated blood to bypass the lungs and mix with oxygenated blood, resulting in cyanosis. The severity depends on the degree of pulmonary stenosis and ventricular septal defect. Surgical repair involves relieving the stenosis and closing the VSD.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Tetrology of fallot
Similar to Tetrology of fallot (20)
More from Rekha Pathak
More from Rekha Pathak (20)
Tetrology of fallot
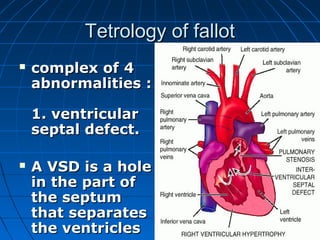
- 1. Tetrology of fallot complex of 4 abnormalities : 1. ventricular septal defect. A VSD is a hole in the part of the septum that separates the ventricles
- 2. hole allows oxygen‑ rich blood to flow from the left ventricle into the right ventricle instead of flowing into the aorta, the main artery leading out to the body
- 3. Pulmonic stenosis 2.Pulmonic stenosis In pulmonary stenosis, the heart has to work harder than normal to pump blood, and not enough blood can get to the lungs.
- 4. 3. The aorta "overrides" the ventricular septal defect. the aorta - between -the left and right ventricles, directly over the VSD. As a result, oxygen‑ poor blood from the right ventricle can flow directly into the aorta instead of into the pulmonary artery to the lungs.
- 5. 4. Thickening (hypertrophy) of the right ventricle Thickening (hypertrophy) of the This is when the right ventricle right ventricle thickens because This is when the right the heart has to ventricle thickens pump harder because the heart has to pump harder than it than it should to should to move blood move blood through the narrowed through the pulmonary valve narrowed pulmonary valve
- 6. Harm Decrease blood flow to lungs Mixing of blood Together, these four defects mean that not enough blood is able to reach the lungs to get oxygen, and oxygen-poor blood flows out to the body.
- 7. Prognosis Despite its seeming complexity, it is quite common and often can be completely repaired.
- 9. THE SERIOUSNESS DEPENDS ON THE DEGREE OF PULMONARY STENOSIS AND VSD MORE THE STENOSIS – MORE BLOOD IS DIVERTED TO LEFT VENTRICLE THROUGH VSD UNOXYGENATED BLOOD TO BODY PARTS BLUISHNESS OF INDIVIDUALS- CYANOSIS IS A CARDINAL SIGN
- 10. SIGNS What are the warning signs and symptoms of Tetralogy of Fallot? Bluish coloring around the mouth, lips, tongue, and fingertips (called cyanosis) DYSPNOEA
- 11. Presence of a heart murmur Occasionally, early on, the degree of Pulmonary Stenosis will be very mild and the symptoms will be that of a Ventricular Septal Defect, including labored breathing, poor feeding, and poor weight gain. Polycyaethemia secondary to hypoxia
- 12. How is Tetralogy of Fallot detected? Heart murmur or Cyanosis. This leads to performing an Cardiac catheterization with angiography is needed prior to surgery to obtain more detailed anatomical information.
- 14. Colour Doppler echo
- 15. Relieving the stenosis Closing the ventricular septal defect by suturing or patch grafting during cardiopulmonary by – pass. Constraints: Size/condition- patient Severity of malformation Lack of cardiopulmonary by pass facilities
- 16. (large concentric hypertrophy of rt. Ventricle and only a narrow slit like lumen of PA- cannot be managed by a closed procedure ) Construction of a palliative shunt – rather than correcting the pulmonary stenosis by a closed technique
- 17. The open-heart repair is then deferred until the patient gets bigger. Less serious TF , have balanced or left to right shunt- and not cyanotic- correcting pulmonary stenosis without correcting VSD is contraindicated
- 18. Palliative shunts Cyanotic – congenital heart disease, polycythemia, history of excessive dyspnea or fainting Subclavean artery with PT (Blalock- Tausssig operation)
- 19. If above not possible- Potts-Smith operation-lt.PA with descending aorta rt.PA with ascending aorta(Waterson shunt) All these – increase blood flow to PA- so spontaneous shunts like PDA in TF – should not be corrected unless hemodyanamics are corrected
- 20. Lobectomy Commonly performed- GA and IPPV Partial/ complete Partial – penetrating wounds – cannot be sutured Complete- pulmonary neoplasms / abscess/cyst/severe lacerations
- 21. Site – depends- -caudal / accessory lobe- 5th or 6th i.c.s. -cranial/middle- 4th /5th ics No noticeable reduction in respiratory function
- 22. Isolate a lobe- hilus is reached- art., bronchus and vein are divided Ligatures with 3-0 silk- vessels
- 23. Lobectomy Area immediately around bronchus – carefully packed off – moist sponges Lobe should be handled as little as possible Cut the shortest possible stump of bronchus Donot apply crushing forecep- stump that is to remain
- 24. Lobectomy After cutting bronchus – a short distance- suture is placed across the edges- prevent escape of air Continue ctting and placing suture- remove the lobe
- 25. Lobectomy Alternatively, hold with rt. Angled foreceps- without crushing- apply 2nd clamp and divide Remove the lobe- close the stump with double row of continuous sutures
- 26. Drip saline during IPPV, - check for air leakage-close the leaks by simple interrupted or matress suture