Download to read offline




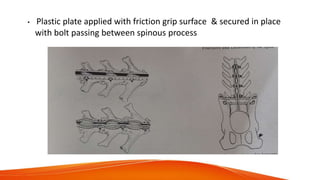
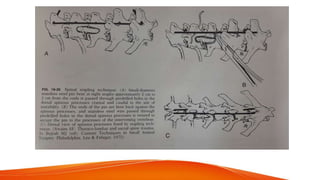










This document provides information on fractures and luxations of the spine in animals. It discusses the intrinsic and extrinsic forces that affect the spine, the anatomy of vertebrae and spinal units, and common sites of fractures. It then describes general treatments for spinal injuries including medications, imaging, and splinting or casting. Surgical techniques for various types of spinal fractures and injuries are outlined, including fixation methods, decompression procedures, and treatment for specific conditions like cervical instability and intervertebral disc disease.










































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











