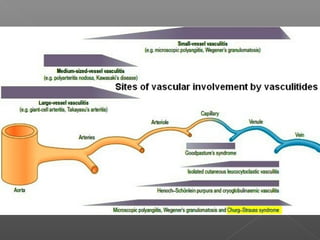
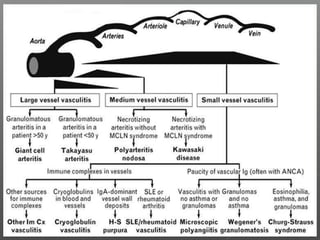
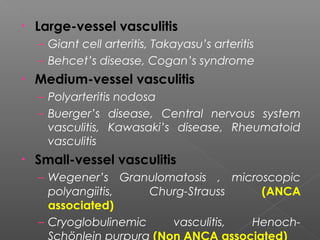
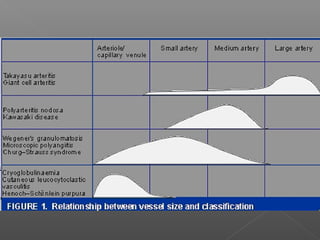
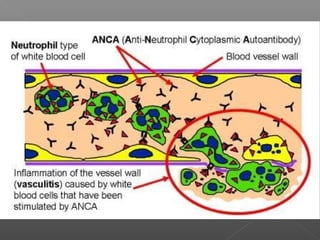
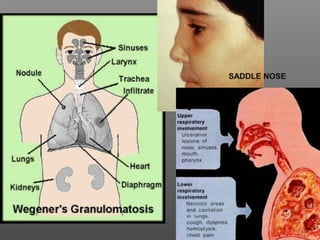
This document discusses vasculitis, which is an inflammatory destruction of blood vessels. It can affect all ages but some types are restricted to certain groups. It has both genetic and environmental components. Symptoms vary depending on the size of vessels involved and can include fatigue, rashes, nerve problems, and organ damage. Diagnosis involves clinical features, lab tests, and sometimes biopsies. Treatment is usually with steroids and other immunosuppressants to induce and maintain remission. Complications can be serious if not treated properly.






































![• Remission induction:
– Cyclophosphamide 2mg/kg po qd x 3-6 months
[or 15 mg/kg IV q 2 wk x3 then q 3 weeks x 6-12 months]
– Prednisone 1mg/kg po qd x 1 month, then taper
– [Bactrim, Calcium, Vitamin D]
• Remission maintenance (minimum 2 years)
– Methotrexate 20-25 mg po q week + folate
– Azathioprine 2mg/kg po qd
– Mycophenolate mofetil 1.5 g po BID
– Leflunomide 20-30 mg po BID](https://image.slidesharecdn.com/vasculitis-140709073318-phpapp02/85/Vasculitis-59-320.jpg)