This document provides information on autoimmune hepatitis, including:
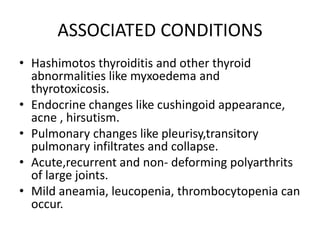
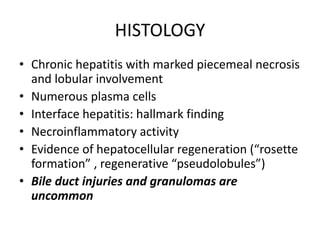
- It is a chronic hepatitis of unknown etiology that can progress to cirrhosis. It is characterized by the presence of autoimmune antibodies and evidence of hepatitis.
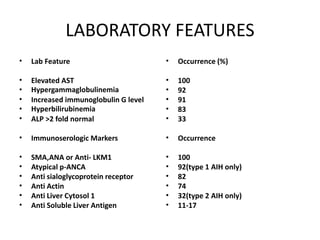
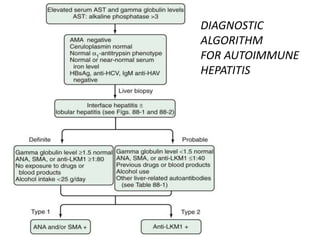
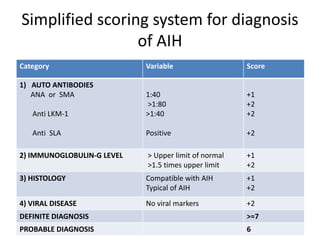
- The two main types are type 1, associated with ANA/SMA positivity, and type 2, associated with LKM1 positivity.
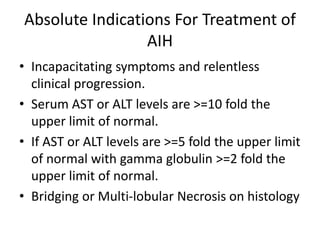
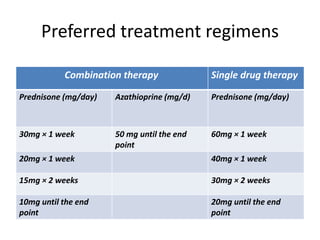
- Treatment involves immunosuppressive drugs like prednisone, either alone or in combination with azathioprine. The goal is to induce and maintain remission.
- Remission is defined as resolution of symptoms and normalization of liver tests and histology. Treatment is then tapered slowly to maintain remission.