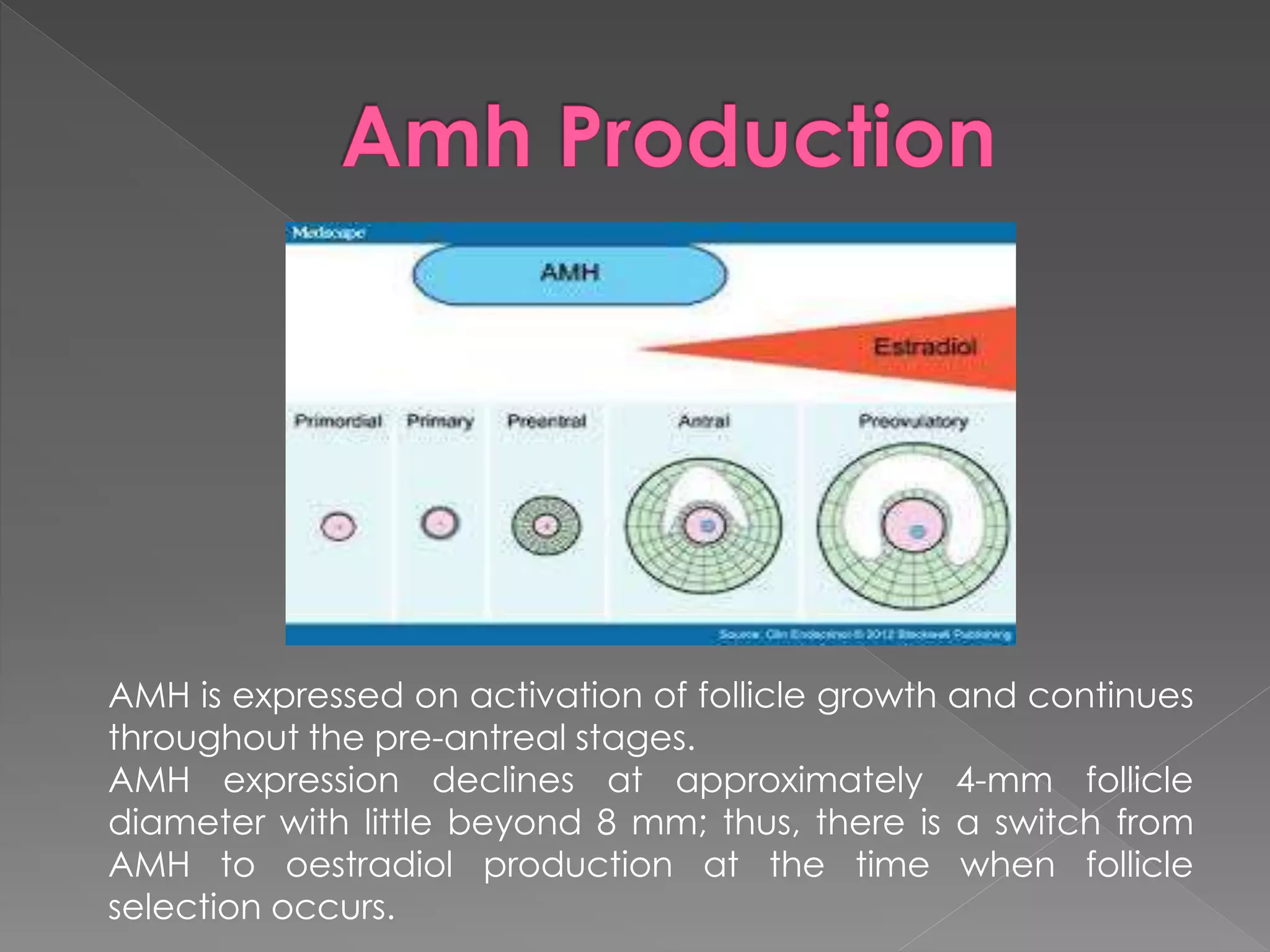
Women's ovarian reserve decreases with age, resulting in infertility around age 40-50. Ovarian reserve reflects the number and quality of eggs and can be assessed through markers like FSH, estradiol, AMH, antral follicle count, and ovarian volume. AMH levels provide the best predictor of ovarian reserve as they fluctuate less than FSH and correlate with antral follicle counts. Both low (<0.5 ng/mL) and high (>2.5 ng/mL) AMH levels impact fertility and IVF outcomes. AMH testing is recommended for women over 30, those with risk factors for low reserve, or who are undergoing fertility treatments.