This document provides an overview of sarcoidosis, including:
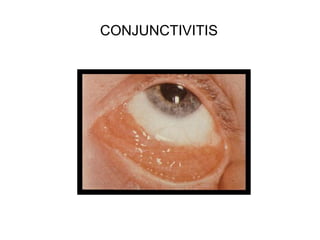
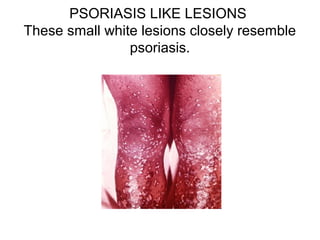
- It is a multisystem granulomatous disorder of unknown cause that commonly affects the lungs, skin and eyes.
- Risk factors include genetics and environmental exposures, and it has the highest rates in the United States and Sweden.
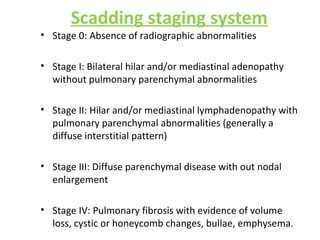
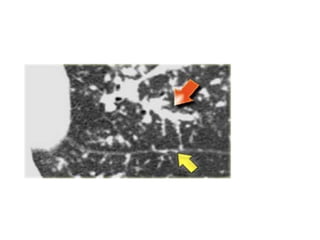
- Clinical presentation varies from asymptomatic to involvement of multiple organ systems. Lung involvement is most common and is staged based on chest x-ray findings.
- Diagnosis involves ruling out other causes and may include biopsy showing non-caseating granulomas. Treatment involves corticosteroids and prognosis is generally good with many experiencing remission.
















![Non-HLA Candidate Genes Evaluated in Sarcoidosis
Vascular endothelial growth factor þ813 CT and TT genotypes associated
with protection
Angiotensin converting enzyme (ACE) Moderate association between II
genotype
C-C Chemokine receptor 2 Associated with protection/Lo ¨ fgren‘s
syndrome
Heat shock protein 70 like HSP(þ2437)CC associated with
susceptibility/Lo ¨ fgren’s syndrome
Vitamin D receptor (VDR BsmI allele associated with sarcoidosis
Cystic fibrosis transmembrane
regulator
(CFTR)
R75Q increases risk
IL1a,IL1 8 The IL-1 a-889 1.1 ; Genotype -607CA
increased risk over AA
Interferon gamma IFNA17 polymorphism (551T!G) and
IFNA10 [60A]- IFNA17 [551G]
haplotype increase risk](https://image.slidesharecdn.com/sarcoidosisfinal-170723174710/85/SARCOIDOSIS-20-320.jpg)