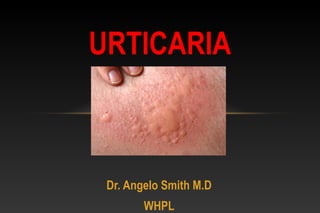
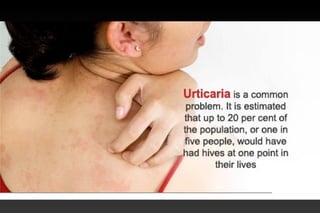
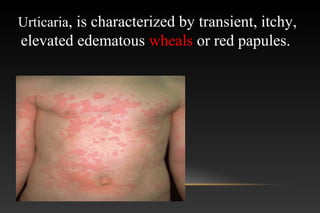
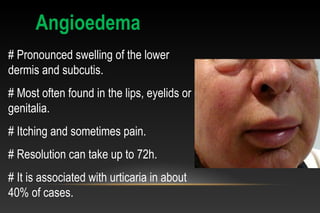
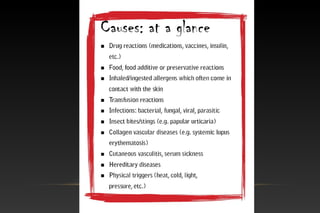
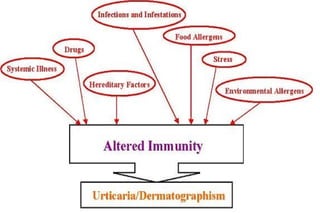
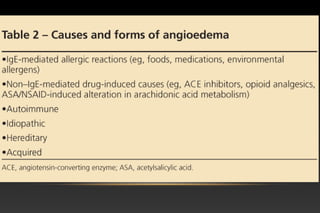
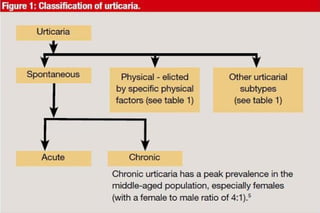
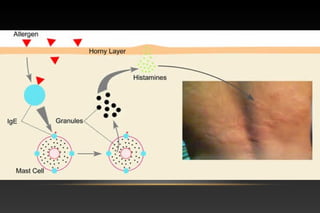
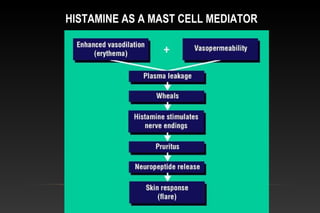
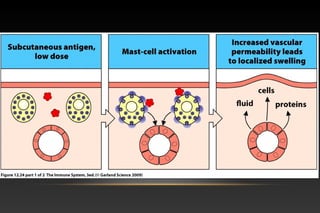
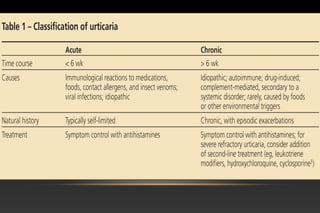
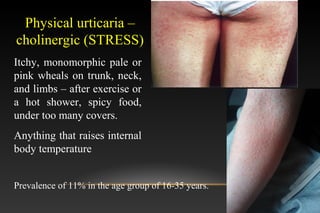
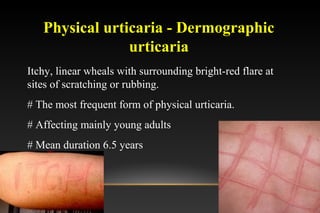
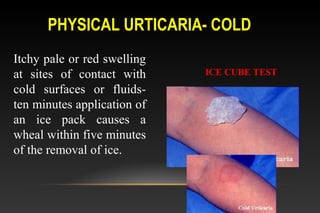
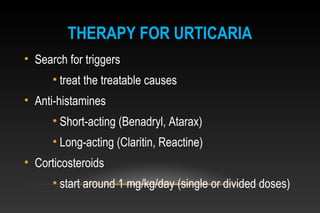
Urticaria, commonly known as hives, is a skin rash with pale red, itchy bumps that appear and disappear quickly. It is characterized by transient wheals (swellings) and angioedema (swelling of deeper layers of skin). Urticaria can be caused by allergic reactions, infections, physical stimuli like heat, cold, pressure, or vibrations. It is classified as acute, chronic, physical or contact urticaria. Treatment involves identifying and avoiding triggers, and using antihistamines.