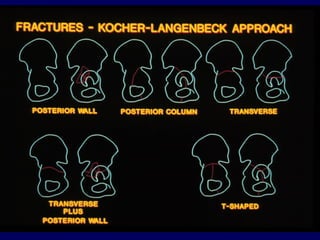
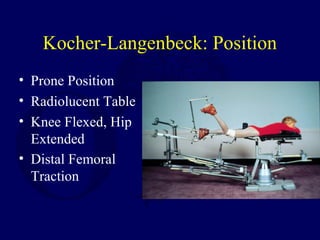
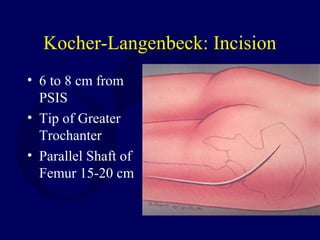
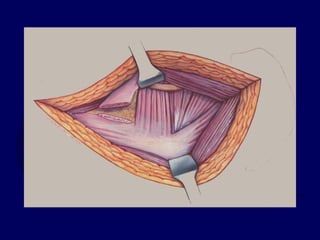
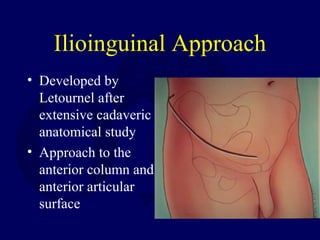
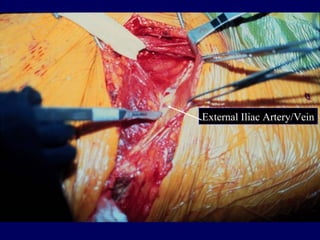
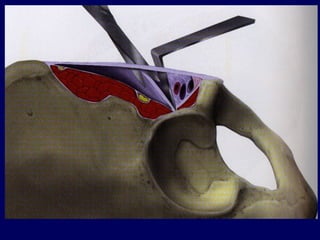
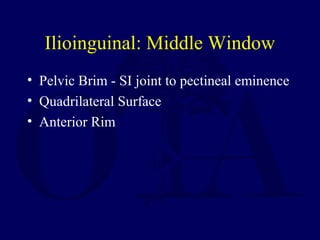
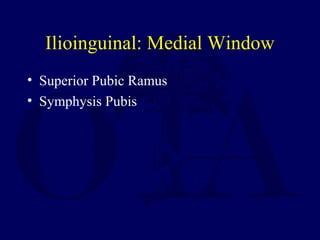
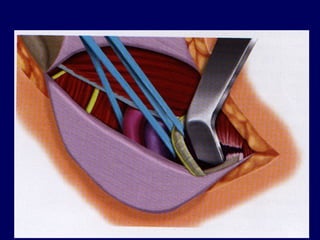
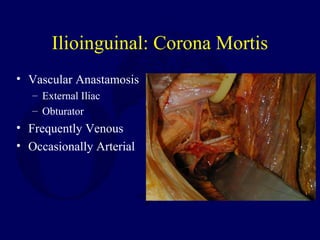
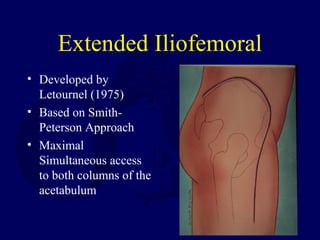
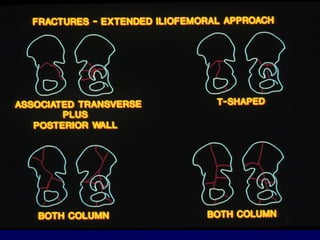
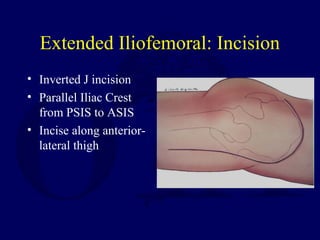
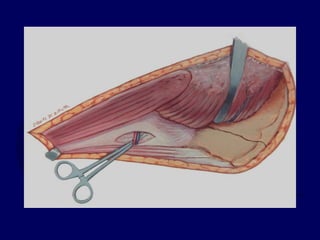
This document describes several surgical approaches for treating fractures of the acetabulum, including the Kocher-Langenbeck, ilioinguinal, and extended iliofemoral approaches. The Kocher-Langenbeck approach is used for posterior column and wall fractures via a posterior incision. The ilioinguinal approach is used for anterior column and wall fractures through an anterior incision. The extended iliofemoral approach provides access to both columns through a lateral incision. Each approach has specific indications, positioning, incisions, dissections, exposures, and potential complications described. Combined approaches may be needed in some complex fracture patterns.























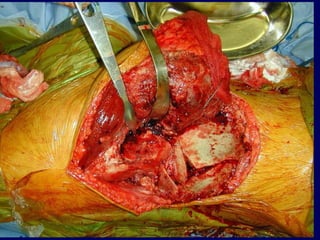





































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
