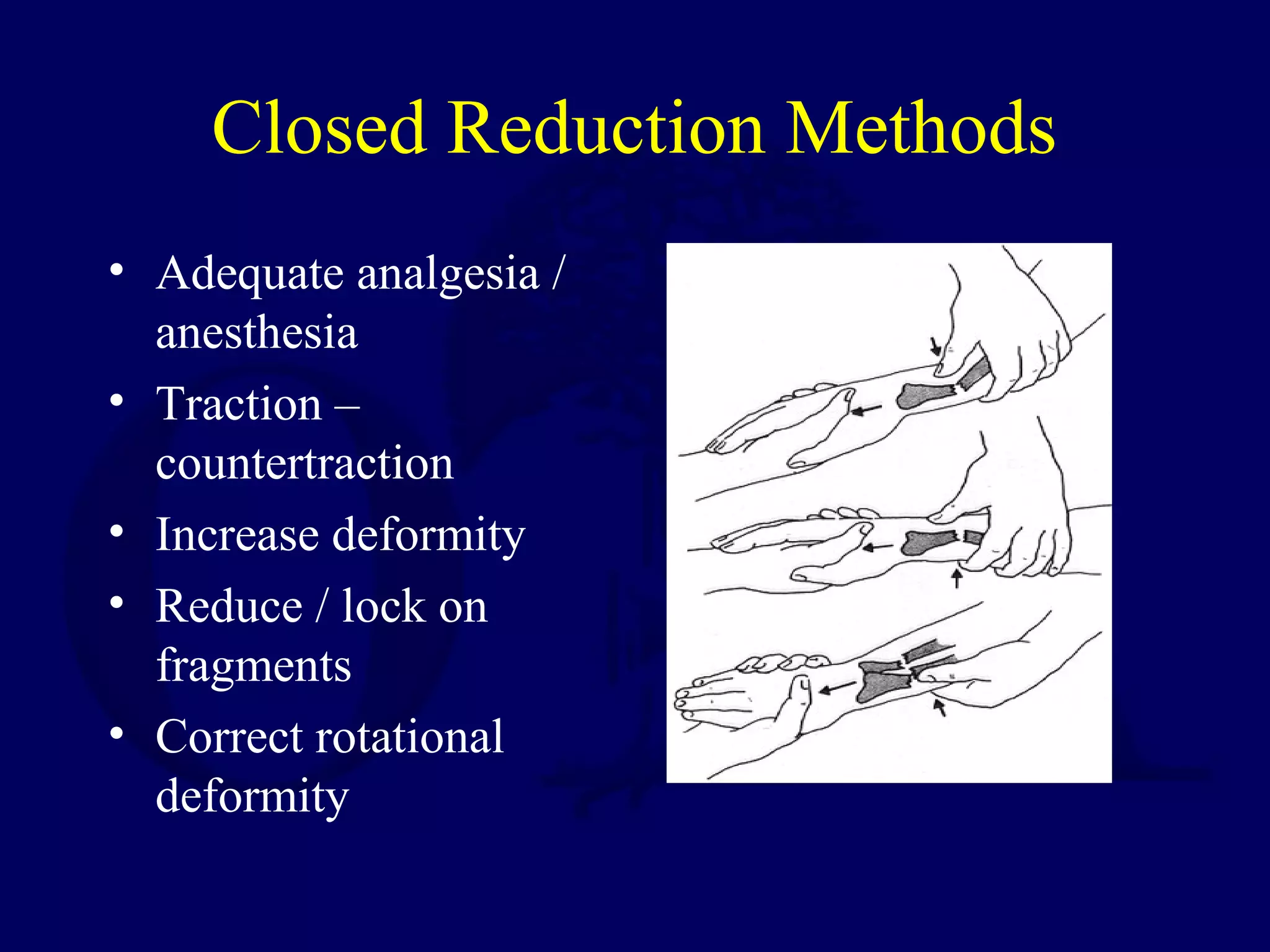
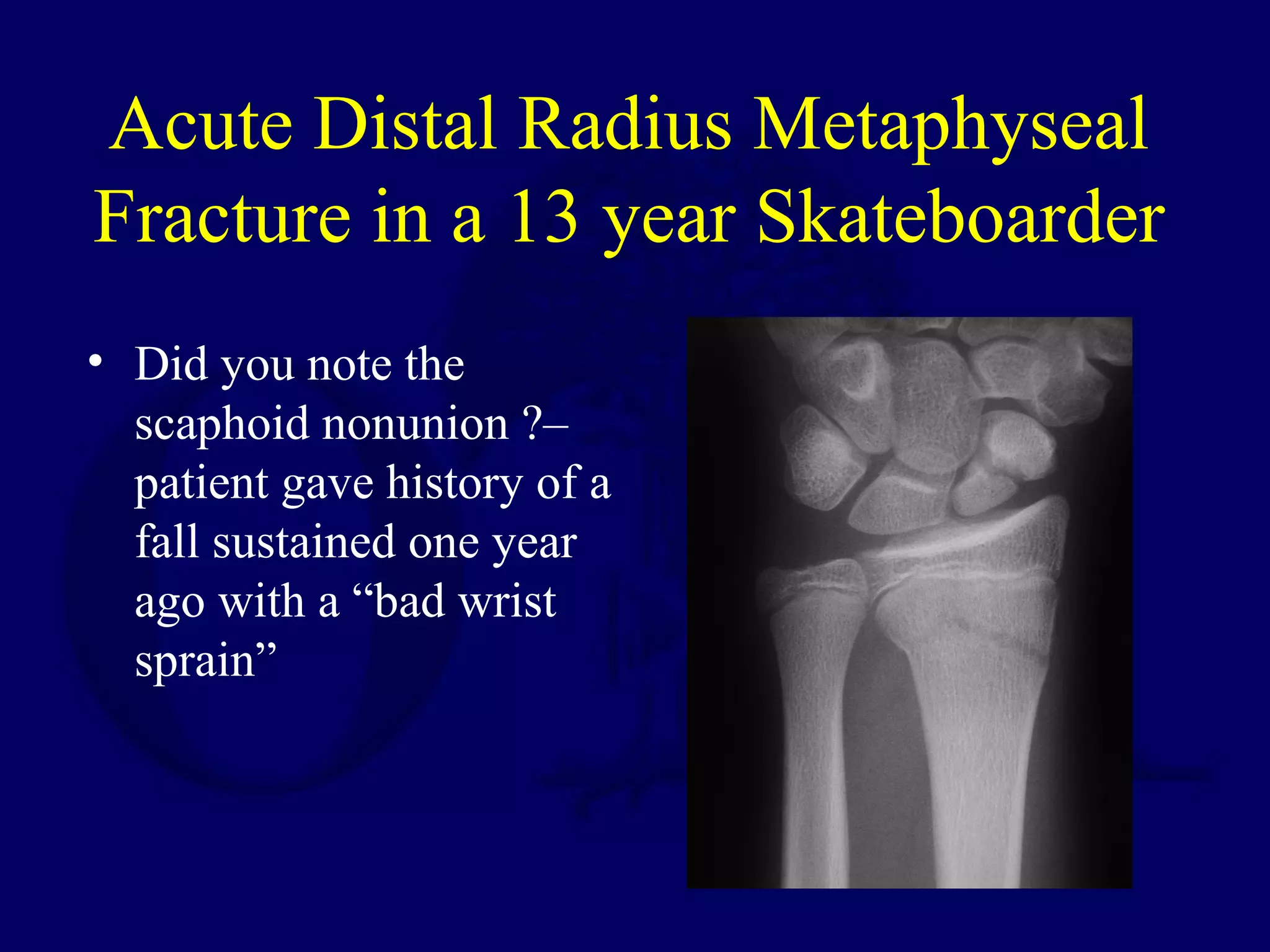
This document discusses pediatric fractures of the forearm, wrist, and hand. It covers topics such as forearm fracture types, anatomy, treatment approaches including closed and open reduction, casting techniques, and complications. Key points include that most forearm fractures can be treated with closed reduction and casting, plastic deformation may limit rotation, distal radius fractures are most common and have good remodeling potential, and scaphoid fractures can lead to nonunion if missed initially.





































































































![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)












































