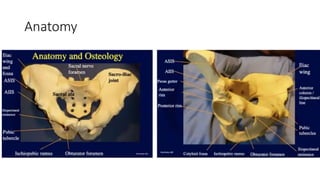
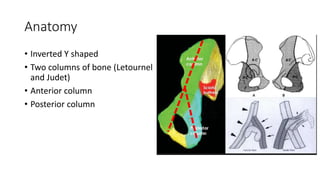
1) Acetabular fractures involve the two columns of bone that make up the acetabulum - the anterior and posterior columns.
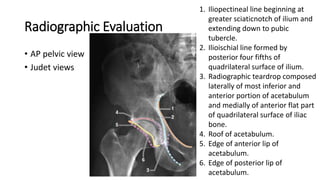
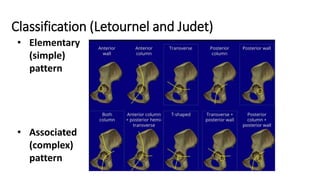
2) Classification systems help determine the best surgical approach and treatment based on which column(s) are fractured and the degree of displacement.
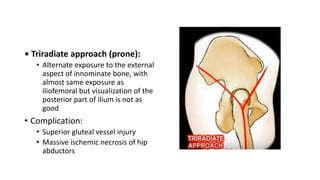
3) Surgical treatment aims to anatomically reduce the articular surface through approaches like the Kocher-Langenbeck or ilioinguinal to place plates and screws, while nonsurgical treatment is indicated for non- or minimally displaced fractures.